Enlarge image
Secretary of the
OFFICE USE ONLY
State of Connecticut
PHONE: 860-509-6003 • EMAIL: crd@ct.gov • WEB: www.concord-sots.ct.gov
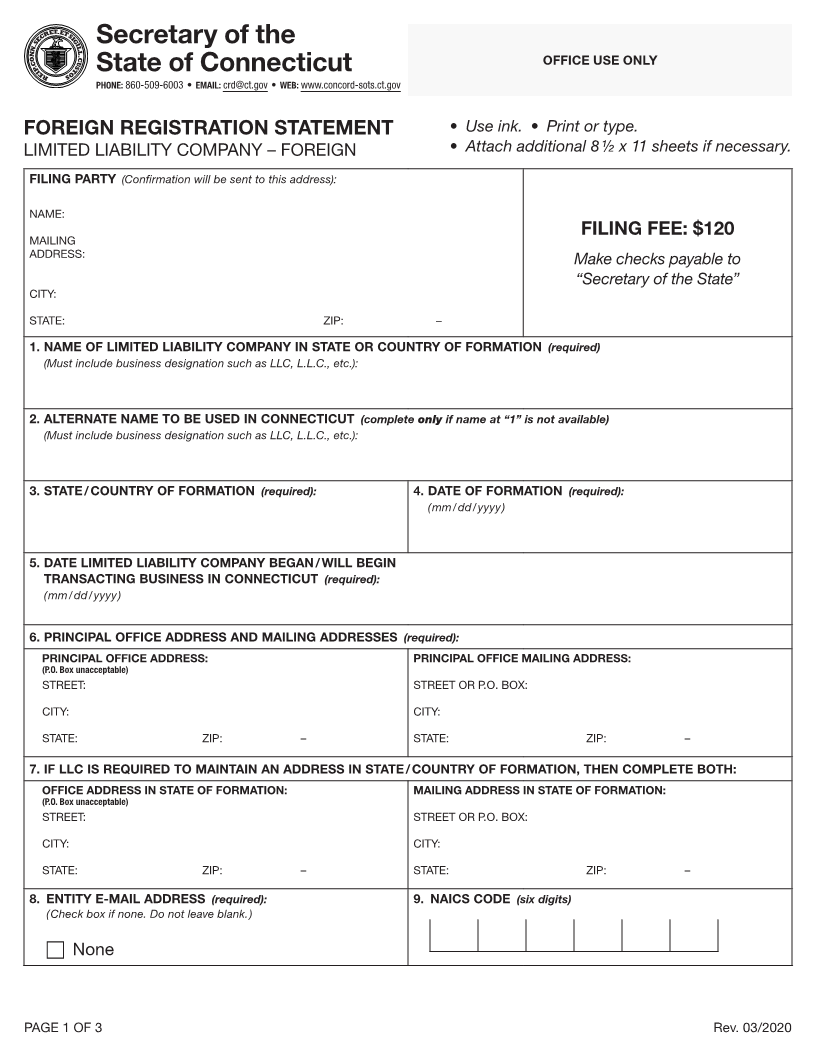
FOREIGN REGISTRATION STATEMENT • Use ink. • Print or type.
LIMITED LIABILITY COMPANY – FOREIGN • Attach additional 8 1/2 x 11 sheets if necessary.
FILING PARTY (Confirmation will be sent to this address):
NAME:
FILING FEE: $120
MAILING
ADDRESS: Make checks payable to
“Secretary of the State”
CITY:
STATE: ZIP: –
1. NAME OF LIMITED LIABILITY COMPANY IN STATE OR COUNTRY OF FORMATION (required)
(Must include business designation such as LLC, L.L.C., etc.):
2. ALTERNATE NAME TO BE USED IN CONNECTICUT (complete only if name at “1” is not available)
(Must include business designation such as LLC, L.L.C., etc.):
3. STATE / COUNTRY OF FORMATION (required): 4. DATE OF FORMATION (required):
( mm / dd / yyyy )
5. DATE LIMITED LIABILITY COMPANY BEGAN / WILL BEGIN
TRANSACTING BUSINESS IN CONNECTICUT (required):
( mm / dd / yyyy )
6. PRINCIPAL OFFICE ADDRESS AND MAILING ADDRESSES (required):
PRINCIPAL OFFICE ADDRESS: PRINCIPAL OFFICE MAILING ADDRESS:
(P.O. Box unacceptable)
STREET: STREET OR P.O. BOX:
CITY: CITY:
STATE: ZIP: – STATE: ZIP: –
7. IF LLC IS REQUIRED TO MAINTAIN AN ADDRESS IN STATE / COUNTRY OF FORMATION, THEN COMPLETE BOTH:
OFFICE ADDRESS IN STATE OF FORMATION: MAILING ADDRESS IN STATE OF FORMATION:
(P.O. Box unacceptable)
STREET: STREET OR P.O. BOX:
CITY: CITY:
STATE: ZIP: – STATE: ZIP: –
8. ENTITY E-MAIL ADDRESS (required): 9. NAICS CODE (six digits)
( Check box if none. Do not leave blank. )
None
PAGE 1 OF 3 Rev. 03/2020