Enlarge image
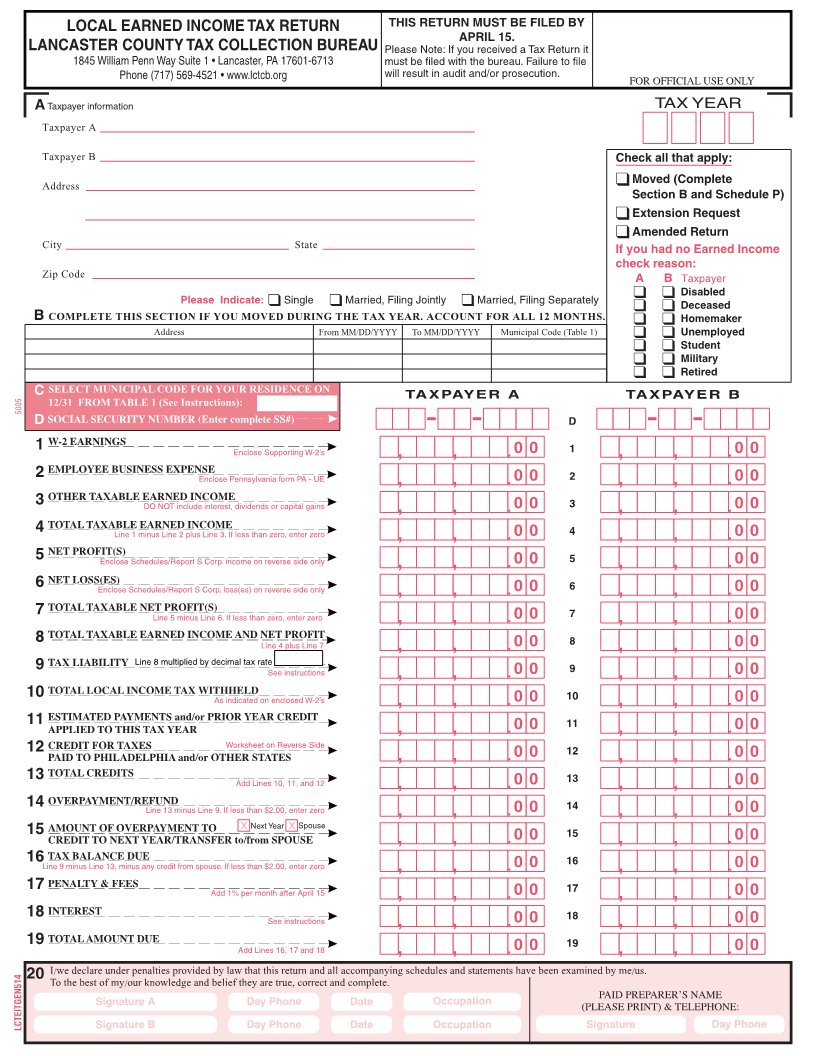
LOCAL EARNED INCOME TAX RETURN THIS RETURN MUST BE FILED BY
APRIL 15.
LANCASTER COUNTY TAX COLLECTION BUREAU Please Note: If you received a Tax Return it
1845 William Penn Way Suite 1 • Lancaster, PA 17601-6713 must be filed with the bureau. Failure to file
Phone (717) 569-4521 • www.lctcb.org will result in audit and/or prosecution.
FOR OFFICIAL USE ONLY
A Taxpayer information TAX YEAR
Taxpayer A
Taxpayer B Check all that apply:
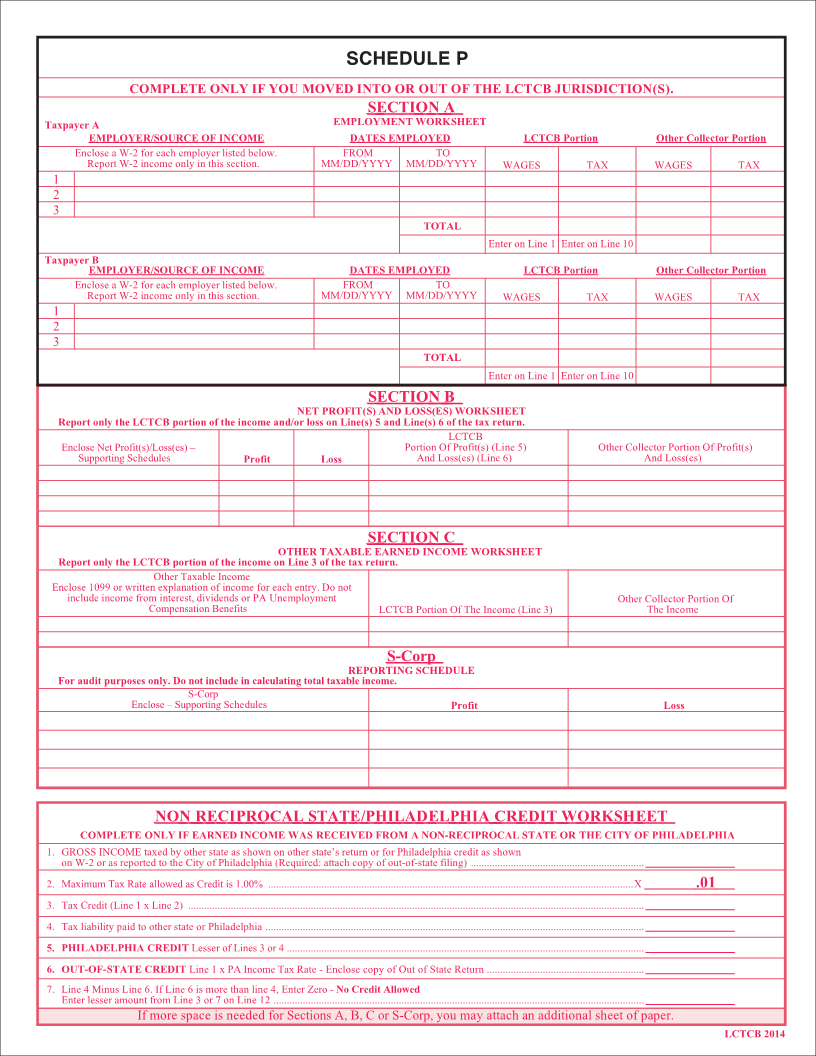
Address Moved (Complete
Section B and Schedule P)
Extension Request
Amended Return
City State If you had no Earned Income
check reason:
Zip Code A B Taxpayer
Disabled
Please Indicate: Single Married, Filing Jointly Married, Filing Separately Deceased
B COMPLETE THIS SECTION IF YOU MOVED DURING THE TAX YEAR. ACCOUNT FOR ALL 12 MONTHS. Homemaker
Address From MM/DD/YYYY To MM/DD/YYYY Municipal Code (Table 1) Unemployed
Student
Military
Retired
C SELECT MUNICIPAL CODE FOR YOUR RESIDENCE ON TAXPAYER A TAXPAYER B
5005 12/31 FROM TABLE 1 (See Instructions):
D SOCIAL SECURITY NUMBER (Enter complete SS#) D
1 W-2 EARNINGS 0 0 1 0 0
Enclose Supporting W-2’s
2 EMPLOYEE BUSINESS EXPENSE 0 0 2 0 0
Enclose Pennsylvania form PA - UE
3 OTHER TAXABLE EARNED INCOME 0 0 3 0 0
DO NOT include interest, dividends or capital gains
4 TOTAL TAXABLE EARNED INCOME 0 0 4 0 0
Line 1 minus Line 2 plus Line 3. If less than zero, enter zero
5 NET PROFIT(S) 0 0 5 0 0
Enclose Schedules/Report S Corp. income on reverse side only
6 NET LOSS(ES) 0 0 6 0 0
Enclose Schedules/Report S Corp. loss(es) on reverse side only
7 TOTAL TAXABLE NET PROFIT(S) 0 0 7 0 0
Line 5 minus Line 6. If less than zero, enter zero
8 TOTAL TAXABLE EARNED INCOME AND NET PROFIT 0 0 8 0 0
Line 4 plus Line 7
9 TAX LIABILITY Line 8 multiplied by decimal tax rate __________. 0 0 0 0
See instructions 9
10 TOTAL LOCAL INCOME TAX WITHHELD 0 0 10 0 0
As indicated on enclosed W-2’s
11 ESTIMATED PAYMENTS and/or PRIOR YEAR CREDIT 0 0 11 0 0
APPLIED TO THIS TAX YEAR
12 CREDIT FOR TAXES Worksheet on Reverse Side 0 0 0 0
12
PAID TO PHILADELPHIA and/or OTHER STATES
13 TOTAL CREDITS 0 0 13 0 0
Add Lines 10, 11, and 12
14 OVERPAYMENT/REFUND 0 0 14 0 0
Line 13 minus Line 9. If less than $2.00, enter zero
15 AMOUNT OF OVERPAYMENT TO Next Year Spouse 0 0 0 0
15
CREDIT TO NEXT YEAR/TRANSFER to/from SPOUSE
16 TAX BALANCE DUE 0 0 16 0 0
Line 9 minus Line 13, minus any credit from spouse. If less than $2.00, enter zero
17 PENALTY & FEES 0 0 17 0 0
Add 1% per month after April 15
18 INTEREST 0 0 18 0 0
See instructions
19 TOTAL AMOUNT DUE 0 0 19 0 0
Add Lines 16, 17 and 18
20 I/we declare under penalties provided by law that this return and all accompanying schedules and statements have been examined by me/us.
To the best of my/our knowledge and belief they are true, correct and complete.
Signature A Day Phone Date Occupation PAID PREPARER’S NAME
(PLEASE PRINT) & TELEPHONE:
LCTEITGEN514 Signature B Day Phone Date Occupation Signature Day Phone