Enlarge image
LOCAL SERVICES TAX – REFUND APPLICATION
___________________________________________
Tax Year
APPLICATION FOR REFUND FROM LOCAL SERVICES TAX
A copy of this application for a refund of the Local Services Tax (LST), and all necessary supporting
documents, must be completed and presented to the tax office charged with collecting the Local Services
Tax.
This application for a refund of the Local Services Tax must be signed and dated.
No refund will be approved until proper documents have been received .
Name: _____________________________________ Soc Sec #: ____________________________________
Address: ___________________________________ Phone #: _____________________________________
City/State: _________________________________ Zip: _________________________________________
REASON FOR REFUND – CHECK ALL THAT APPLY
1.__________ I overpaid by more than $1.
2.__________ I had the tax withheld when it should have been exempted.
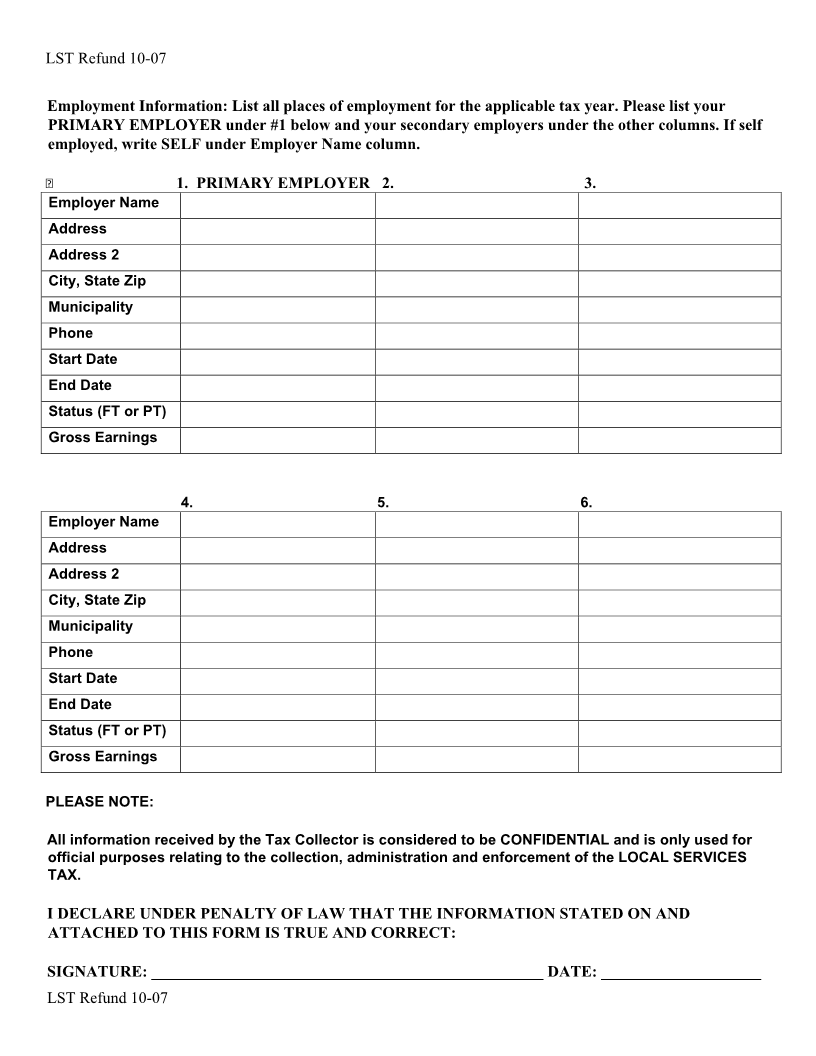
3.__________ MULTIPLE EMPLOYERS: Please attach a copy of a current pay statement from your
principal employer that shows the name of the employer, the length of the payroll period and the amount of
Local Services Tax withheld. Please list all employers on the reverse side of this form.
4.__________ TOTAL EARNED INCOME AND NET PROFITS FROM ALL SOURCES WITHIN
_____________________________________ (municipality or school district) WAS
LESS THAN $_____________: Please attach a copy of all of your last pay statements
from all employers within the political subdivision for the year prior to the fiscal year for
which you are requesting to be exempted from the Local Services Tax.
If you are self-employed, please attach a copy of your PA Schedule C, F, or RK-1 for the
year prior to the fiscal year for which you are requesting to receive a refund of the Local
Services Tax.
5.__________ ACTIVE DUTY MILITARY EXEMPTION: Please attach a copy of your orders
directing you to active duty status.
6.__________ MILITARY DISABILITY EXEMPTION: Please attach copy of your discharge orders
and a statement from the United States Veterans Administrator or its successor declaring your disability to be
a total one hundred percent permanent disability.
Tax Office: Berkheimer Tax Innovations
Address: PO Box 25156 Phone #: (610) 588-0965
City/State: Lehigh Valley, PA Zip: 18002