Enlarge image
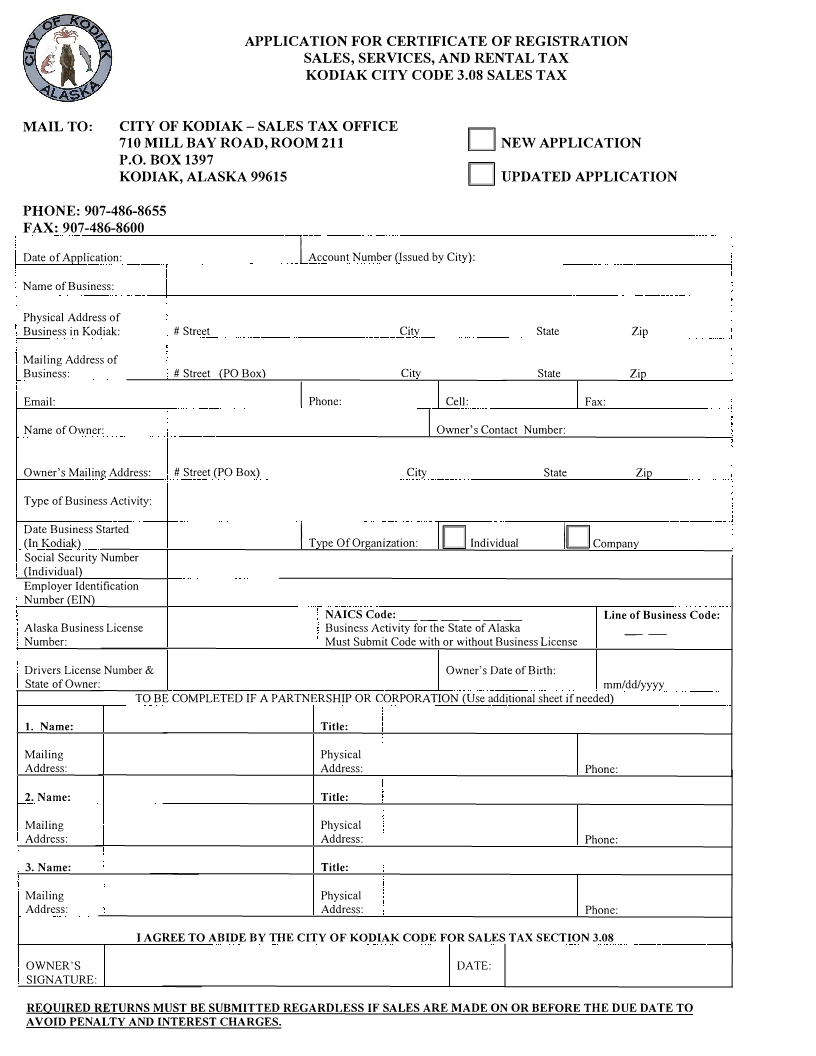
APPLICATION FOR CERTIFICATE OF REGISTRATION
SALES, SERVICES, AND RENTAL TAX
KODIAK CITY CODE 3.08 SALES TAX
MAIL TO: CITY OF KODIAK- SALES TAX OFFICE
710 MILL BAY ROAD, ROOM 211 D NEW APPLICATION
P.O. BOX 1397
KODIAK, ALASKA 99615 D UPDATED APPLICATION
PHONE: 907-486-8655
FAX: 907-486-8600
Date of Application: Account Number (Issued bv Citv):
I
Name of Business:
Physical Address of
Business in Kodiak: # Street Citv State Zip
Mailing Address of
Business: # Street (PO Box) Citv State Zio
Email: Phone: Cell: Fax:
I
Name of Owner: Owner's Contact Number:
I
Owner's Mailing Address: # Street (PO Box) City State Zip
Type of Business Activity:
Date Business Started
(In Kodiak) Type Of Organization: D Individual ID Comoanv
Social Security Number I
(Individual)
Employer Identification
Number (EIN)
NAICSCode: ------ Line of Business Code:
Alaska Business License Business Activity for the State of Alaska --
Number: Must Submit Code with or without Business License
Drivers License Number & Owner's Date of Birth:
State of Owner: mm/dd/yyyy
TO BE COMPLETED IF A PARTNERSHIP OR CORPORATION (Use additional sheet if needed)
I. Name: Title:
Mailing Physical
Address: Address: Phone:
2. Name: Title:
Mailing Physical
Address: Address: Phone:
3. Name: Title:
Mailing Physical
Address: Address: Phone:
I AGREE TO ABIDE BY THE CITY OF KODIAK CODE FOR SALES TAX SECTION 3.08
OWNER'S DATE:
SIGNATURE:
REQUIRED RETURNS MUST BE SUBMITTED REGARDLESS IF SALES ARE MADE ON OR BEFORE THE DUE DATE TO
A VOID PENALTY AND INTEREST CHARGES.