Enlarge image
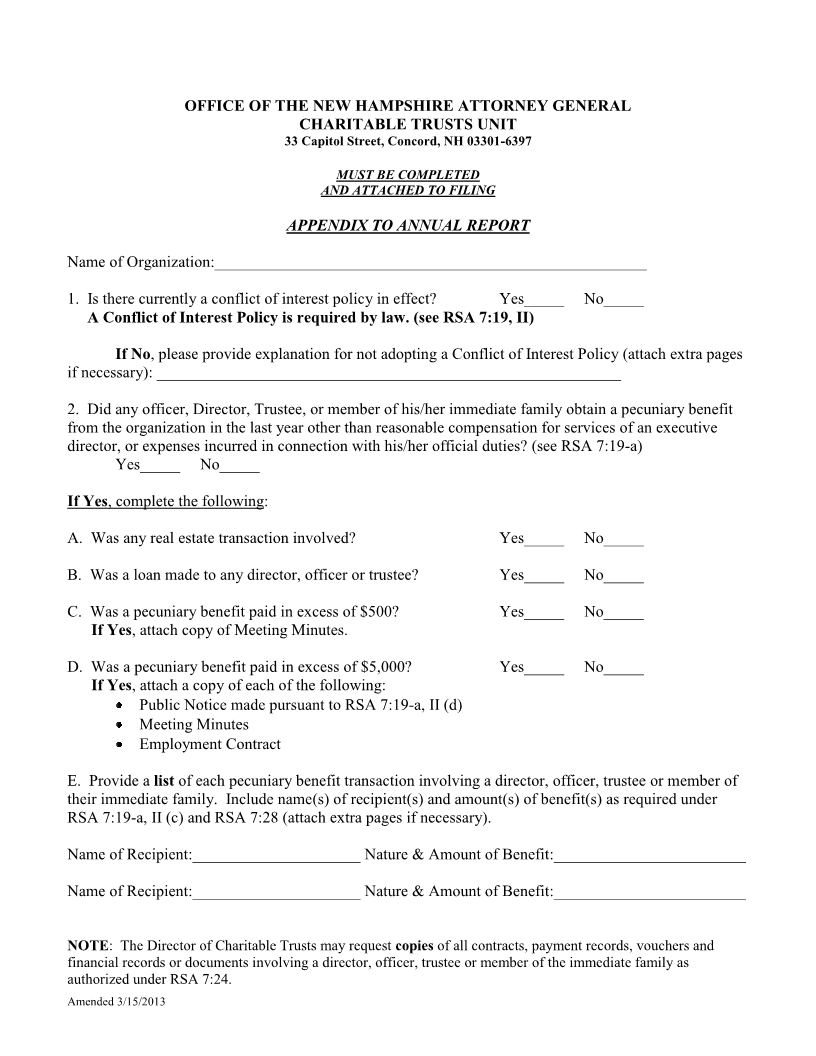
OFFICE OF THE NEW HAMPSHIRE ATTORNEY GENERAL
CHARITABLE TRUSTS UNIT
33 Capitol Street, Concord, NH 03301-6397
MUST BE COMPLETED
AND ATTACHED TO FILING
APPENDIX TO ANNUAL REPORT
Name of Organization:______________________________________________________
1. Is there currently a conflict of interest policy in effect? Yes_____ No_____
A Conflict of Interest Policy is required by law. (see RSA 7:19, II)
If No, please provide explanation for not adopting a Conflict of Interest Policy (attach extra pages
if necessary): __________________________________________________________
2. Did any officer, Director, Trustee, or member of his/her immediate family obtain a pecuniary benefit
from the organization in the last year other than reasonable compensation for services of an executive
director, or expenses incurred in connection with his/her official duties? (see RSA 7:19-a)
Yes_____ No_____
If Yes, complete the following:
A. Was any real estate transaction involved? Yes_____ No_____
B. Was a loan made to any director, officer or trustee? Yes_____ No_____
C. Was a pecuniary benefit paid in excess of $500? Yes_____ No_____
If Yes, attach copy of Meeting Minutes.
D. Was a pecuniary benefit paid in excess of $5,000? Yes_____ No_____
If Yes, attach a copy of each of the following:
Public Notice made pursuant to RSA 7:19-a, II (d)
Meeting Minutes
Employment Contract
E. Provide a list of each pecuniary benefit transaction involving a director, officer, trustee or member of
their immediate family. Include name(s) of recipient(s) and amount(s) of benefit(s) as required under
RSA 7:19-a, II (c) and RSA 7:28 (attach extra pages if necessary).
Name of Recipient:_____________________ Nature & Amount of Benefit:________________________
Name of Recipient:_____________________ Nature & Amount of Benefit:________________________
NOTE: The Director of Charitable Trusts may request copies of all contracts, payment records, vouchers and
financial records or documents involving a director, officer, trustee or member of the immediate family as
authorized under RSA 7:24.
Amended 3/15/2013