Enlarge image
SCHEDULE H OMB No. 1545-0047
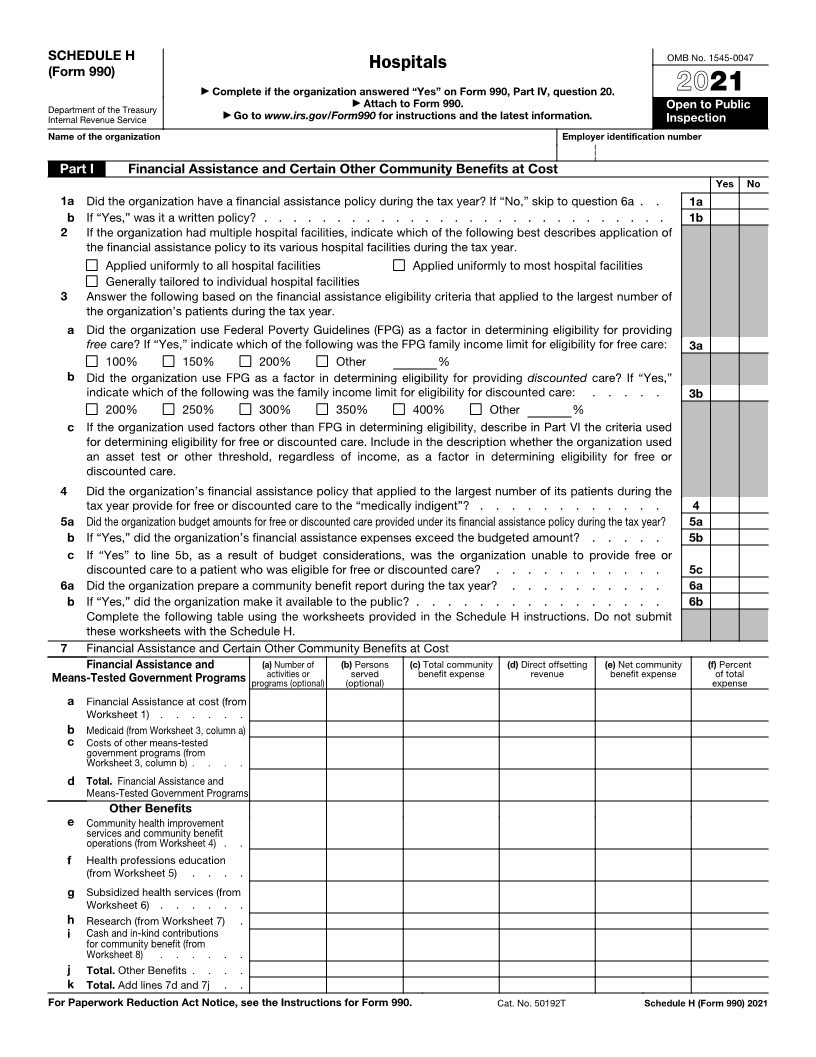
(Form 990) Hospitals
▶ Complete if the organization answered “Yes” on Form 990, Part IV, question 20. 2021
▶
Department of the Treasury Attach to Form 990. Open to Public
Internal Revenue Service ▶ Go to www.irs.gov/Form990 for instructions and the latest information. Inspection
Name of the organization Employer identification number
Part I Financial Assistance and Certain Other Community Benefits at Cost
Yes No
1a Did the organization have a financial assistance policy during the tax year? If “No,” skip to question 6a . . 1a
b If “Yes,” was it a written policy? . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1b
2 If the organization had multiple hospital facilities, indicate which of the following best describes application of
the financial assistance policy to its various hospital facilities during the tax year.
Applied uniformly to all hospital facilities Applied uniformly to most hospital facilities
Generally tailored to individual hospital facilities
3 Answer the following based on the financial assistance eligibility criteria that applied to the largest number of
the organization’s patients during the tax year.
a Did the organization use Federal Poverty Guidelines (FPG) as a factor in determining eligibility for providing
free care? If “Yes,” indicate which of the following was the FPG family income limit for eligibility for free care: 3a
100% 150% 200% Other %
b Did the organization use FPG as a factor in determining eligibility for providing discounted care? If “Yes,”
indicate which of the following was the family income limit for eligibility for discounted care: . . . . . 3b
200% 250% 300% 350% 400% Other %
c If the organization used factors other than FPG in determining eligibility, describe in Part VI the criteria used
for determining eligibility for free or discounted care. Include in the description whether the organization used
an asset test or other threshold, regardless of income, as a factor in determining eligibility for free or
discounted care.
4 Did the organization’s financial assistance policy that applied to the largest number of its patients during the
tax year provide for free or discounted care to the “medically indigent”? . . . . . . . . . . . . 4
5a Did the organization budget amounts for free or discounted care provided under its financial assistance policy during the tax year? 5a
b If “Yes,” did the organization’s financial assistance expenses exceed the budgeted amount? . . . . . 5b
c If “Yes” to line 5b, as a result of budget considerations, was the organization unable to provide free or
discounted care to a patient who was eligible for free or discounted care? . . . . . . . . . . . 5c
6a Did the organization prepare a community benefit report during the tax year? . . . . . . . . . . 6a
b If “Yes,” did the organization make it available to the public? . . . . . . . . . . . . . . . . 6b
Complete the following table using the worksheets provided in the Schedule H instructions. Do not submit
these worksheets with the Schedule H.
7 Financial Assistance and Certain Other Community Benefits at Cost
Financial Assistance and (a) Number of (b) Persons (c) Total community (d) Direct offsetting (e) Net community (f) Percent
Means-Tested Government Programsactivities or served benefit expense revenue benefit expense of total
programs (optional)(optional) expense
a Financial Assistance at cost (from
Worksheet 1) . . . . . .
b Medicaid (from Worksheet 3, column a)
c Costs of other means-tested
government programs (from
Worksheet 3, column b) . . . .
d Total. Financial Assistance and
Means-Tested Government Programs
Other Benefits
e Community health improvement
services and community benefit
operations (from Worksheet 4) . .
f Health professions education
(from Worksheet 5) . . . .
g Subsidized health services (from
Worksheet 6) . . . . . .
h Research (from Worksheet 7) .
i Cash and in-kind contributions
for community benefit (from
Worksheet 8) . . . . . .
j Total. Other Benefits . . . .
k Total. Add lines 7d and 7j . .
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Cat. No. 50192T Schedule H (Form 990) 2021