Enlarge image
OMB Control No: 0970-0166
OMB Expiration Date: 07/31/2025
Multistate Employer Registration Form for
New Hire Reporting
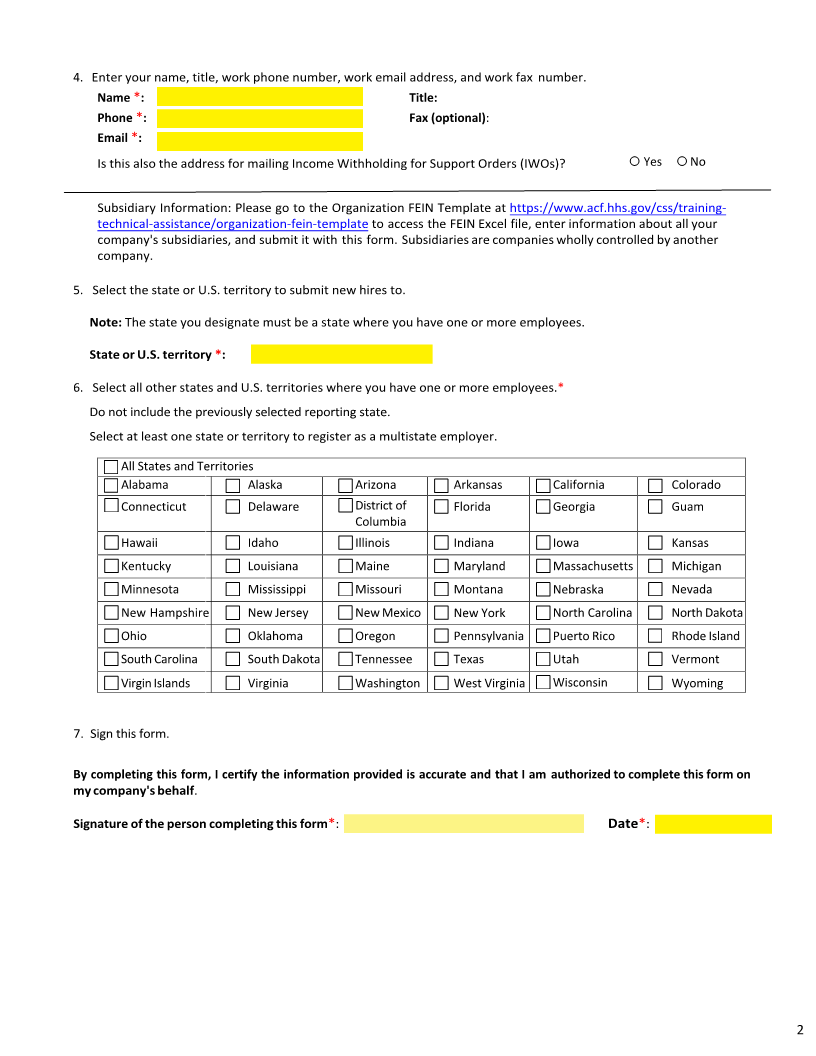
Employers who have employees working in two or more states may use this form to register to submit their new hire
reports to one state or make changes to a previous registration. Multistate employers may register online at
https://ocsp.acf.hhs.gov/OCSE/.
Note: If you are a third-party provider, your clients must have employees in two or more states to register as a
multistate employer.
Federal law (42 U.S.C. § 653A(b)(1)(A)) requires employers to supply the following information about newly hired
employees to the State Directory of New Hires in the state where the employee works:
■ Employee's name, address, Social Security number, and the date of hire (the date services for remuneration
were first performed by the employee)
■ Employer's name, address, and Federal Employer Identification Number (FEIN)
If you are an employer with employees working in two or more states, and you will transmit the required information or
reports magnetically or electronically, you can use this form to designate one state where any employee works to transmit all
new hire reports to the State Directory of New Hires.
If you are no longer a multistate employer or you are a multistate employer but no longer report to a single state, select the No
Longer a Multistate Employer check box below.
No Longer a Multistate Employer (If selected, complete items 1–4 and 7) and return the form to the email address
msedb@acf.hhs.gov or mail it to the address located on page 3.
If you need help completing this form, contact the Multistate Employer Help Desk at 800-258-2736 (8 a.m. – 5 p.m. ET,
Monday through Friday).
Note: All required fields are followed by a red asterisk .*
1. Enter your company's FEIN without a hyphen. 2. Enter today's date in MM/DD/YYYY format.
This is the nine-digit number used by the IRS to
identify your company.
FEIN *: Date :*
3. Enter your company's legal name used for child support documents. This is the name associated with the FEIN in
item 1.
Employer Name :*
Enter your company's address, including city, state, and ZIP code. This is the address associated with the FEIN in
item 1. If your company's FEIN address is a foreign address, enter the country's name and postal code.
Employer Address *:
City :* State *:
ZIP Code *:
(For foreign addresses only) Country Name: Country Postal Code:
1