Enlarge image
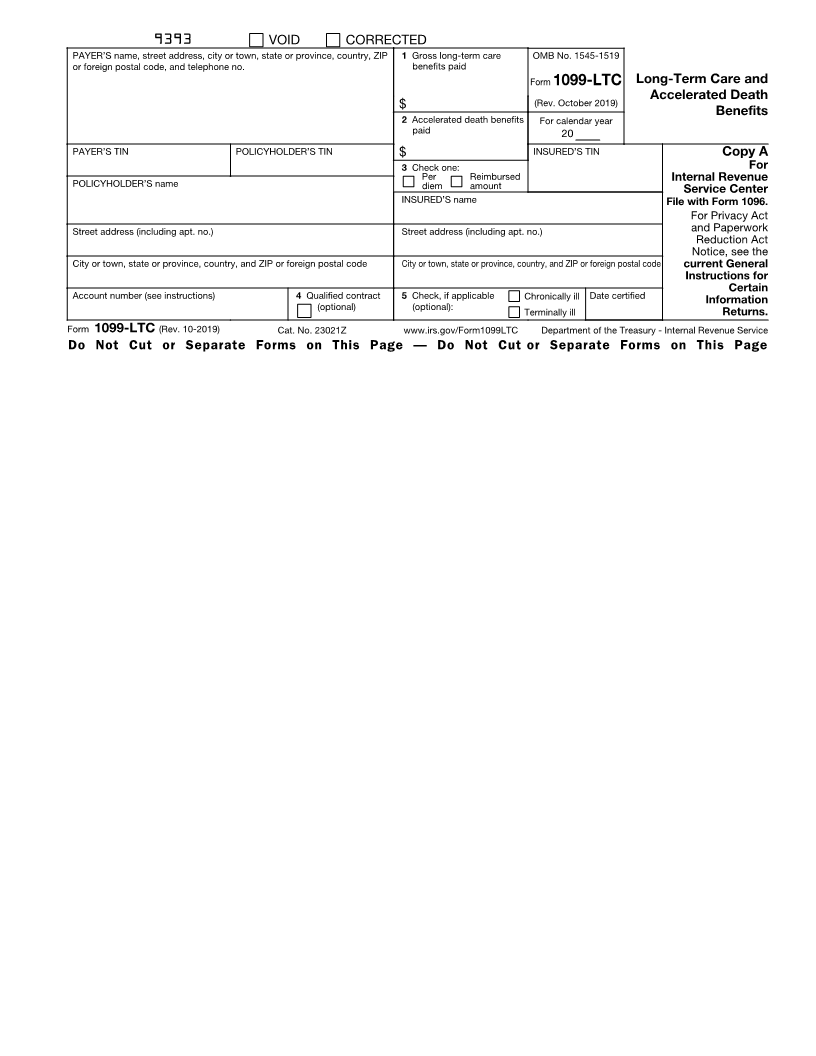
9393 VOID CORRECTED
PAYER’S name, street address, city or town, state or province, country, ZIP 1 Gross long-term care OMB No. 1545-1519
or foreign postal code, and telephone no. benefits paid
Form 1099-LTC Long-Term Care and
(Rev. October 2019) Accelerated Death
$
Benefits
2 Accelerated death benefits For calendar year
paid 20
PAYER’S TIN POLICYHOLDER’S TIN $ INSURED’S TIN Copy A
3 Check one: For
Per Reimbursed
POLICYHOLDER’S name diem amount Internal Revenue
Service Center
INSURED’S name File with Form 1096.
For Privacy Act
Street address (including apt. no.) Street address (including apt. no.) and Paperwork
Reduction Act
Notice, see the
City or town, state or province, country, and ZIP or foreign postal code City or town, state or province, country, and ZIP or foreign postal code current General
Instructions for
Certain
Account number (see instructions) 4 Qualified contract 5 Check, if applicable Chronically ill Date certified Information
(optional) (optional): Terminally ill Returns.
Form 1099-LTC (Rev. 10-2019) Cat. No. 23021Z www.irs.gov/Form1099LTC Department of the Treasury - Internal Revenue Service
Do Not Cut or Separate Forms on This Page — Do Not Cut or Separate Forms on This Page