Enlarge image
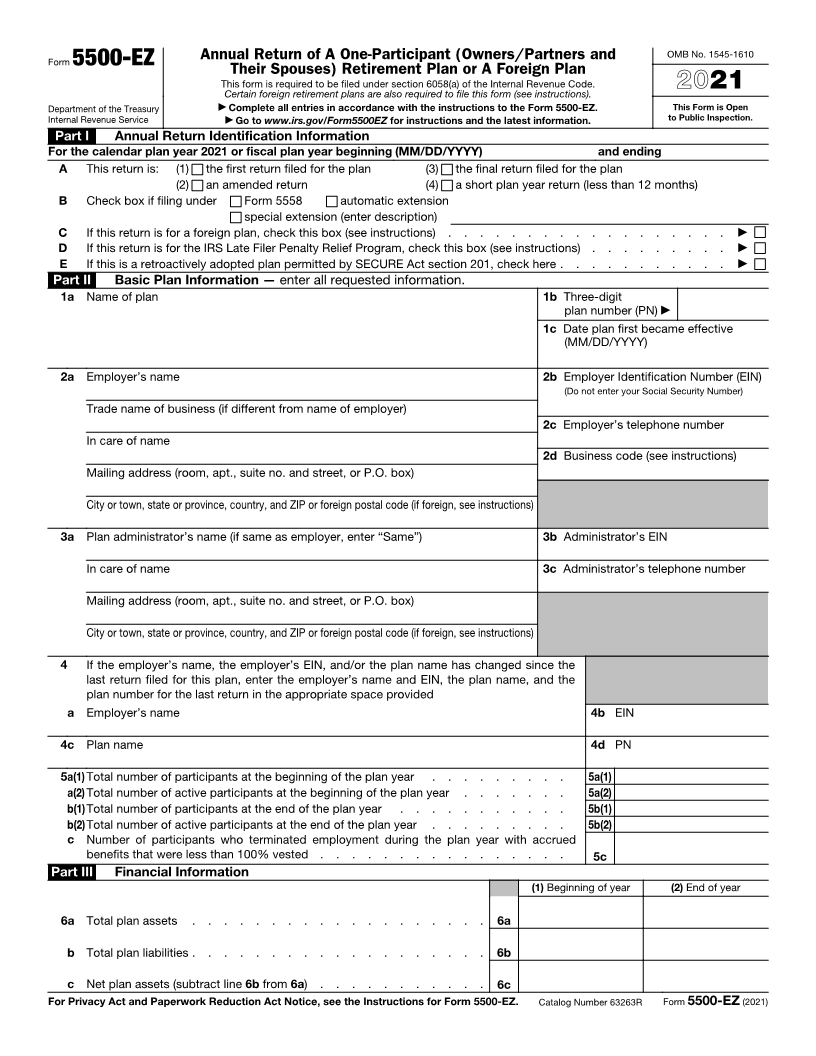
Annual Return of A One-Participant (Owners/Partners and OMB No. 1545-1610
Form 5500-EZ
Their Spouses) Retirement Plan or A Foreign Plan
This form is required to be filed under section 6058(a) of the Internal Revenue Code. 2021
Certain foreign retirement plans are also required to file this form (see instructions).
Department of the Treasury ▶ Complete all entries in accordance with the instructions to the Form 5500-EZ. This Form is Open
Internal Revenue Service ▶ Go to www.irs.gov/Form5500EZ for instructions and the latest information. to Public Inspection.
Part I Annual Return Identification Information
For the calendar plan year 2021 or fiscal plan year beginning (MM/DD/YYYY) and ending
A This return is: (1) the first return filed for the plan (3) the final return filed for the plan
(2) an amended return (4) a short plan year return (less than 12 months)
B Check box if filing under Form 5558 automatic extension
special extension (enter description)
C If this return is for a foreign plan, check this box (see instructions) . . . . . . . . . . . . . . . . . . ▶
D If this return is for the IRS Late Filer Penalty Relief Program, check this box (see instructions) . . . . . . . . . ▶
E If this is a retroactively adopted plan permitted by SECURE Act section 201, check here . . . . . . . . . . . ▶
Part II Basic Plan Information — enter all requested information.
1a Name of plan 1b Three-digit
plan number (PN) ▶
1c Date plan first became effective
(MM/DD/YYYY)
2a Employer’s name 2b Employer Identification Number (EIN)
(Do not enter your Social Security Number)
Trade name of business (if different from name of employer)
2c Employer’s telephone number
In care of name
2d Business code (see instructions)
Mailing address (room, apt., suite no. and street, or P.O. box)
City or town, state or province, country, and ZIP or foreign postal code (if foreign, see instructions)
3a Plan administrator’s name (if same as employer, enter “Same”) 3b Administrator’s EIN
In care of name 3c Administrator’s telephone number
Mailing address (room, apt., suite no. and street, or P.O. box)
City or town, state or province, country, and ZIP or foreign postal code (if foreign, see instructions)
4 If the employer’s name, the employer’s EIN, and/or the plan name has changed since the
last return filed for this plan, enter the employer’s name and EIN, the plan name, and the
plan number for the last return in the appropriate space provided
a Employer’s name 4b EIN
4c Plan name 4d PN
5a(1) Total number of participants at the beginning of the plan year . . . . . . . . . 5a(1)
a(2) Total number of active participants at the beginning of the plan year . . . . . . . 5a(2)
b(1)Total number of participants at the end of the plan year . . . . . . . . . . . 5b(1)
b(2)Total number of active participants at the end of the plan year . . . . . . . . . 5b(2)
c Number of participants who terminated employment during the plan year with accrued
benefits that were less than 100% vested . . . . . . . . . . . . . . . . 5c
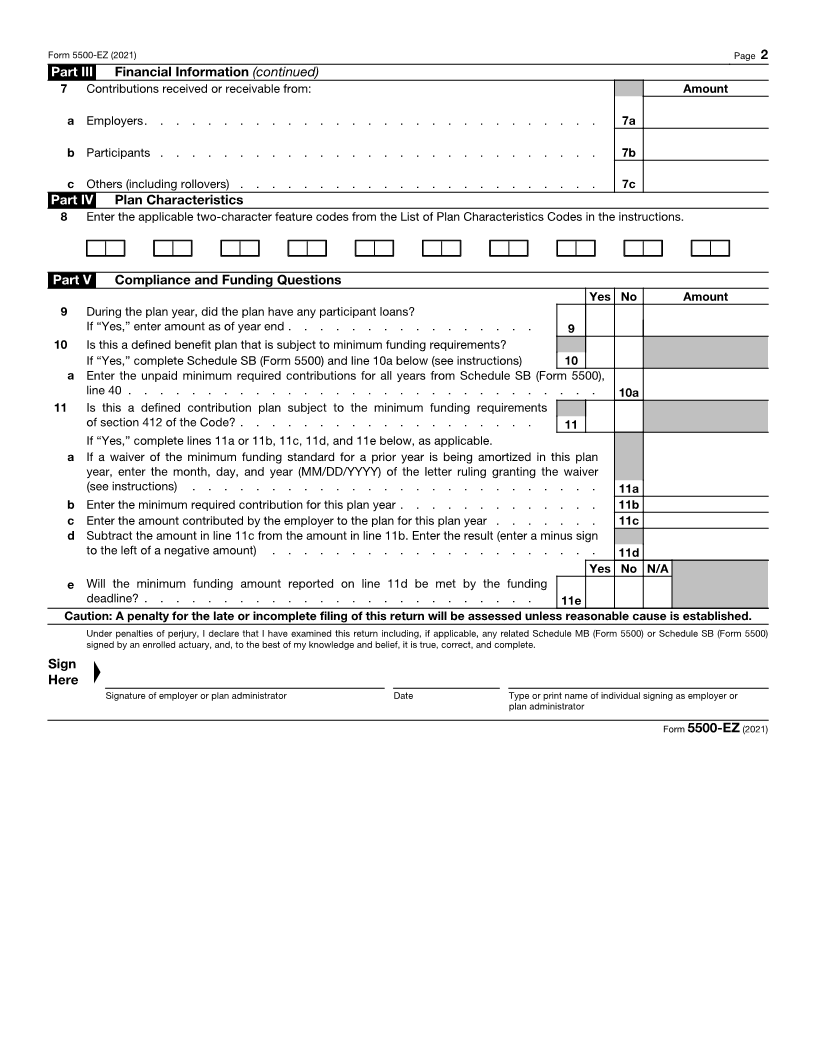
Part III Financial Information
(1) Beginning of year (2) End of year
6a Total plan assets . . . . . . . . . . . . . . . . . . . 6a
b Total plan liabilities . . . . . . . . . . . . . . . . . . . 6b
c Net plan assets (subtract line 6b from 6a) . . . . . . . . . . . 6c
For Privacy Act and Paperwork Reduction Act Notice, see the Instructions for Form 5500-EZ. Catalog Number 63263R Form 5500-EZ (2021)