Enlarge image
Reset Form Print Form
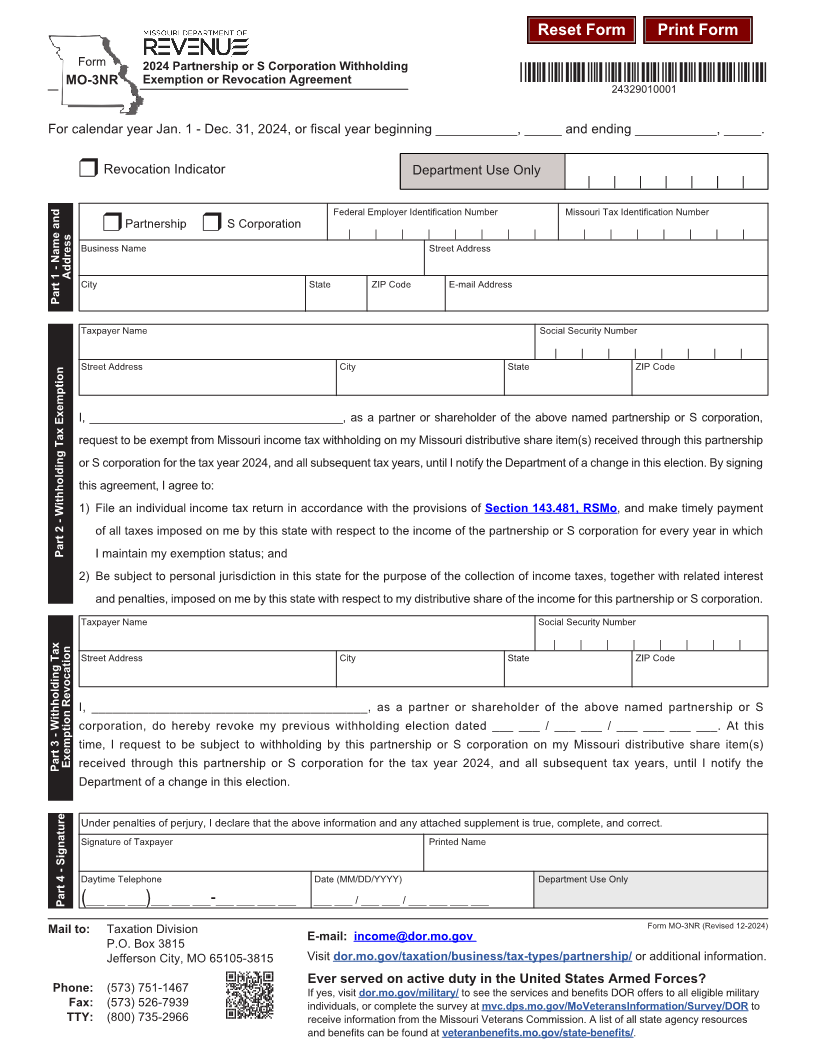
Form 2024 Partnership or S Corporation Withholding
Exemption or Revocation Agreement *24329010001*
MO-3NR
24329010001
For calendar year Jan. 1 - Dec. 31, 2024, or fiscal year beginning ___________, _____ and ending ___________, _____.
r Revocation Indicator Department Use Only
| | | | | | |
Federal Employer Identification Number Missouri Tax Identification Number
r Partnership r S Corporation
| | | | | | | | | | | | | | |
Business Name Street Address
Address
City State ZIP Code E-mail Address
Part 1 - Name and
Taxpayer Name Social Security Number
| | | | | | | |
Street Address City State ZIP Code
I, _______________________________________, as a partner or shareholder of the above named partnership or S corporation,
request to be exempt from Missouri income tax withholding on my Missouri distributive share item(s) received through this partnership
or S corporation for the tax year 2024, and all subsequent tax years, until I notify the Department of a change in this election. By signing
this agreement, I agree to:
1) File an individual income tax return in accordance with the provisions of Section 143.481, RSMo, and make timely payment
of all taxes imposed on me by this state with respect to the income of the partnership or S corporation for every year in which
Part 2 - Withholding Tax Exemption I maintain my exemption status; and
2) Be subject to personal jurisdiction in this state for the purpose of the collection of income taxes, together with related interest
and penalties, imposed on me by this state with respect to my distributive share of the income for this partnership or S corporation.
Taxpayer Name Social Security Number
| | | | | | | |
Street Address City State ZIP Code
I, _______________________________________, as a partner or shareholder of the above named partnership or S
corporation, do hereby revoke my previous withholding election dated ___ ___ / ___ ___ / ___ ___ ___ ___. At this
time, I request to be subject to withholding by this partnership or S corporation on my Missouri distributive share item(s)
Part 3 - Withholding Tax Exemption Revocation received through this partnership or S corporation for the tax year 2024, and all subsequent tax years, until I notify the
Department of a change in this election.
Under penalties of perjury, I declare that the above information and any attached supplement is true, complete, and correct.
Signature of Taxpayer Printed Name
Daytime Telephone Date (MM/DD/YYYY) Department Use Only
Part(___4 -___Signature___) ___ ___ ___-___ ___ ___ ___ ___ ___ / ___ ___ / ___ ___ ___ ___
Mail to: Taxation Division Form MO-3NR (Revised 12-2024)
E-mail: income@dor.mo.gov
P.O. Box 3815
Jefferson City, MO 65105-3815 Visit dor.mo.gov/taxation/business/tax-types/partnership/ or additional information.
Ever served on active duty in the United States Armed Forces?
Phone: (573) 751-1467 If yes, visit dor.mo.gov/military/ to see the services and benefits DOR offers to all eligible military
Fax: (573) 526-7939 individuals, or complete the survey at mvc.dps.mo.gov/MoVeteransInformation/Survey/DOR to
TTY: (800) 735-2966 receive information from the Missouri Veterans Commission. A list of all state agency resources
and benefits can be found at veteranbenefits.mo.gov/state-benefits/.