Enlarge image
1 1
1 2 2 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 Form All layers With grid &2 data 84 85
3 4 82 83
3 3
4 4
5 Oregon Department of Revenue 5
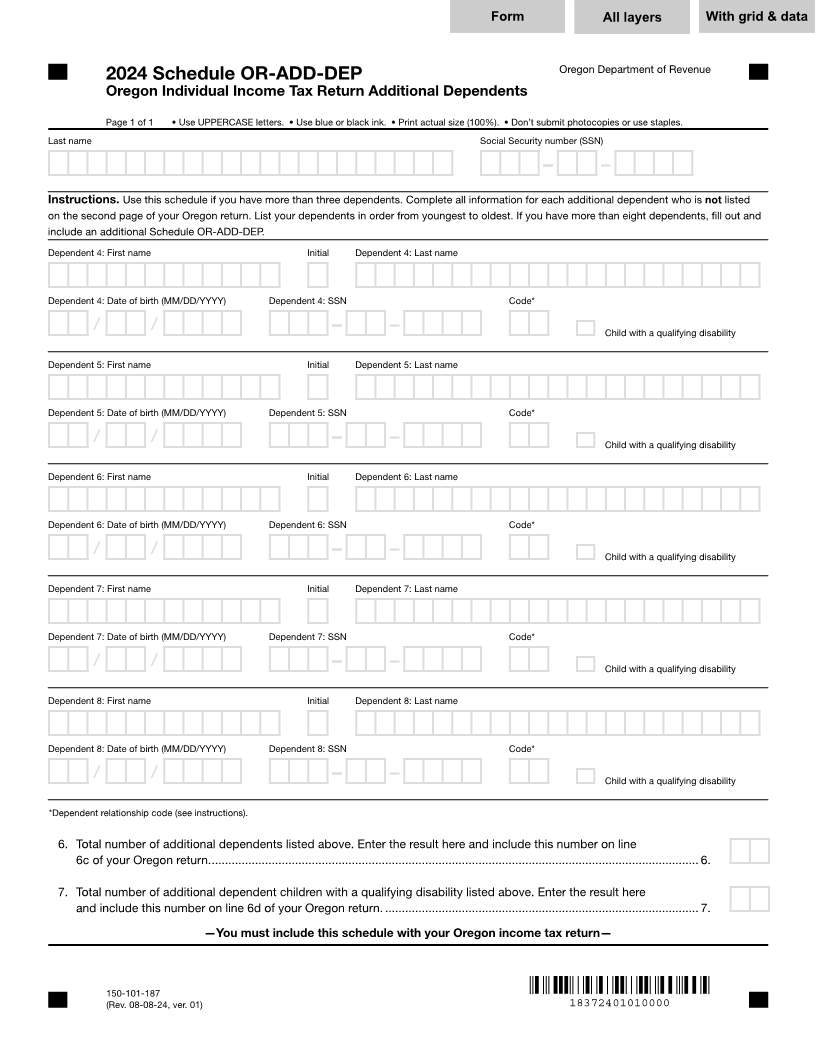
2024 Schedule OR-ADD-DEP
6 Oregon Individual Income Tax Return Additional Dependents 6
7 7
8 Page 1 of 1 • Use UPPERCASE letters. • Use blue or black ink. • Print actual size (100%). • Don’t submit photocopies or use staples. 8
9 Last name Social Security number (SSN) 9
10 10
11 11
XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 999-99-9999
12 12
13 Instructions. Use this schedule if you have more than three dependents. Complete all information for each additional dependent who is not listed 13
14 on the second page of your Oregon return. List your dependents in order from youngest to oldest. If you have more than eight dependents, fill out and 14
15 include an additional Schedule OR-ADD-DEP. 15
16 Dependent 4: First name Initial Dependent 4: Last name 16
17 17
18 18
XXXXXXXXXXXXXXXX X XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
19 Dependent 4: Date of birth (MM/DD/YYYY) Dependent 4: SSN Code* 19
20 20
21 99/99/9999/ / 999-99-9999 XX X Child with a qualifying disability 21
22 22
23 Dependent 5: First name Initial Dependent 5: Last name 23
24 24
25 25
XXXXXXXXXXXXXXXX X XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
26 Dependent 5: Date of birth (MM/DD/YYYY) Dependent 5: SSN Code* 26
27 27
28 99/99/9999/ / 999-99-9999 XX X Child with a qualifying disability 28
29 29
30 Dependent 6: First name Initial Dependent 6: Last name 30
31 31
32 32
XXXXXXXXXXXXXXXX X XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
33 Dependent 6: Date of birth (MM/DD/YYYY) Dependent 6: SSN Code* 33
34 34
35 99/99/9999/ / 999-99-9999 XX X Child with a qualifying disability 35
36 36
37 Dependent 7: First name Initial Dependent 7: Last name 37
38 38
39 39
XXXXXXXXXXXXXXXX X XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
40 Dependent 7: Date of birth (MM/DD/YYYY) Dependent 7: SSN Code* 40
41 41
42 99/99/9999/ / 999-99-9999 XX X Child with a qualifying disability 42
43 43
44 Dependent 8: First name Initial Dependent 8: Last name 44
45 45
46 46
XXXXXXXXXXXXXXXX X XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
47 Dependent 8: Date of birth (MM/DD/YYYY) Dependent 8: SSN Code* 47
48 48
49 99/99/9999/ / 999-99-9999 XX X Child with a qualifying disability 49
50 50
51 *Dependent relationship code (see instructions). 51
52 52
53 6. Total number of additional dependents listed above. Enter the result here and include this number on line 53
54 6c of your Oregon return. .................................................................................................................................................. 6. 99 54
55 55
56 7. Total number of additional dependent children with a qualifying disability listed above. Enter the result here 56
57 and include this number on line 6d of your Oregon return. .............................................................................................. 7. 99 57
58 58
59 —You must include this schedule with your Oregon income tax return— 59
60 60
61 61
62 62
150-101-187
63 (Rev. 08-08-24, ver. 01) 18372401010000 63
64 64
1 2 65 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 65 84 85
3 4 82 83
66 66