Enlarge image
1 1
1 2 2 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 Form With grid With grid & data2 84 85
3 4 82 83
3 3
4 4
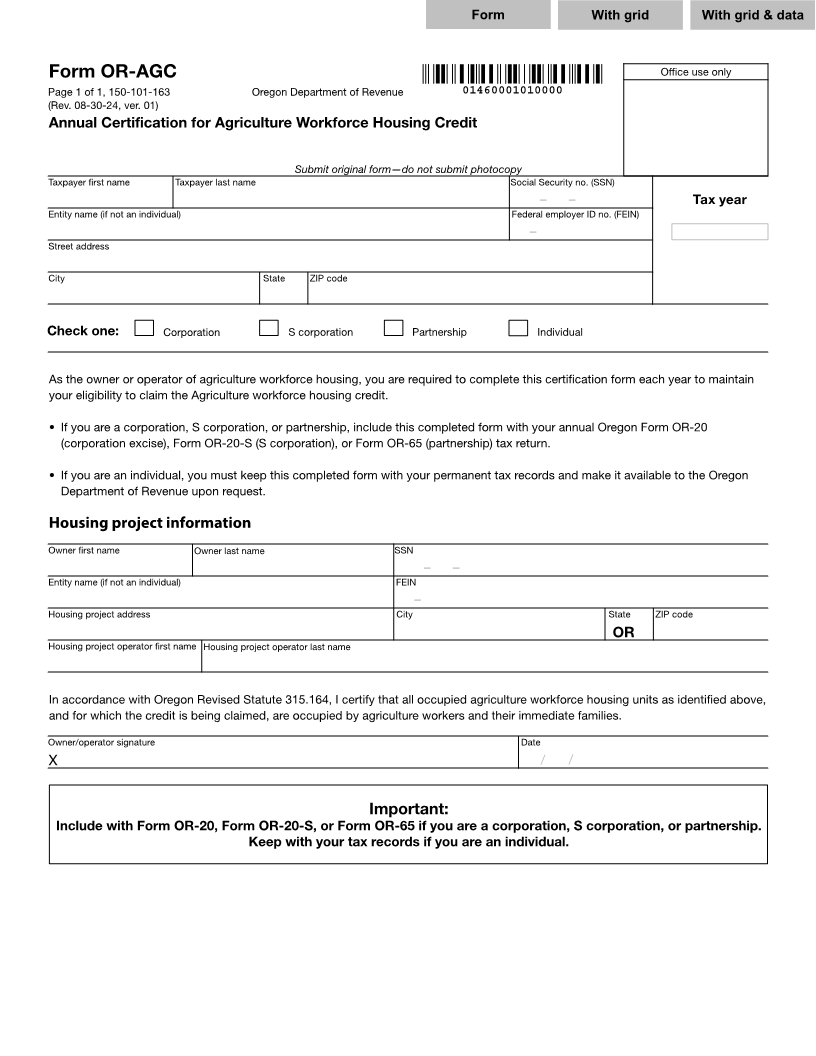
5 Form OR-AGC Office use only 5
6 Page 1 of 1, 150-101-163 Oregon Department of Revenue 01460001010000 6
7 (Rev. 08-30-24, ver. 01) 7
8 Annual Certification for Agriculture Workforce Housing Credit 8
9 9
10 10
11 Submit original form—do not submit photocopy 11
12 Taxpayer first name Taxpayer last name Social Security no. (SSN) 12
13 XXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXX 999-99-9999– – Tax year 13
14 Entity name (if not an individual) Federal employer ID no. (FEIN) 14
15 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 99-9999999– 9999 15
16 Street address 16
17 17
18 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXCity State ZIP code 18
19 19
XXXXXXXXXXXXXXXXXXXXX XX XXXXX-XXXX
20 20
21 Check one: X Corporation X S corporation X Partnership X Individual 21
22 22
23 23
24 As the owner or operator of agriculture workforce housing, you are required to complete this certification form each year to maintain 24
25 your eligibility to claim the Agriculture workforce housing credit. 25
26 26
27 • If you are a corporation, S corporation, or partnership, include this completed form with your annual Oregon Form OR-20 27
28 (corporation excise), Form OR-20-S (S corporation), or Form OR-65 (partnership) tax return. 28
29 29
30 • If you are an individual, you must keep this completed form with your permanent tax records and make it available to the Oregon 30
31 Department of Revenue upon request. 31
32 32
33 33
Housing project information
34 34
35 Owner first name Owner last name SSN 35
36 XXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXX999-99-9999– – 36
37 Entity name (if not an individual) FEIN 37
38 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 99-9999999– 38
39 Housing project address City State ZIP code 39
40 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXXX OR XXXXX-XXXX 40
41 Housing project operator first name Housing project operator last name 41
42 42
XXXXXXXXXXXX XXXXXXXXXXXXXXXXXXXX
43 43
44 In accordance with Oregon Revised Statute 315.164, I certify that all occupied agriculture workforce housing units as identified above, 44
45 and for which the credit is being claimed, are occupied by agriculture workers and their immediate families. 45
46 46
47 Owner/operator signature Date 47
48 X 99/99/9999/ / 48
49 49
50 50
51 Important: 51
52 Include with Form OR-20, Form OR-20-S, or Form OR-65 if you are a corporation, S corporation, or partnership. 52
53 Keep with your tax records if you are an individual. 53
54 54
55 55
56 56
57 57
58 58
59 59
60 60
61 61
62 62
63 63
64 64
1 2 65 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 65 84 85
3 4 82 83
66 66