Enlarge image
1 1
1 2 2 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 Form All layers With grid &2 data 84 85
3 4 82 83
3 3
4 4
5 Oregon Department of Revenue 5
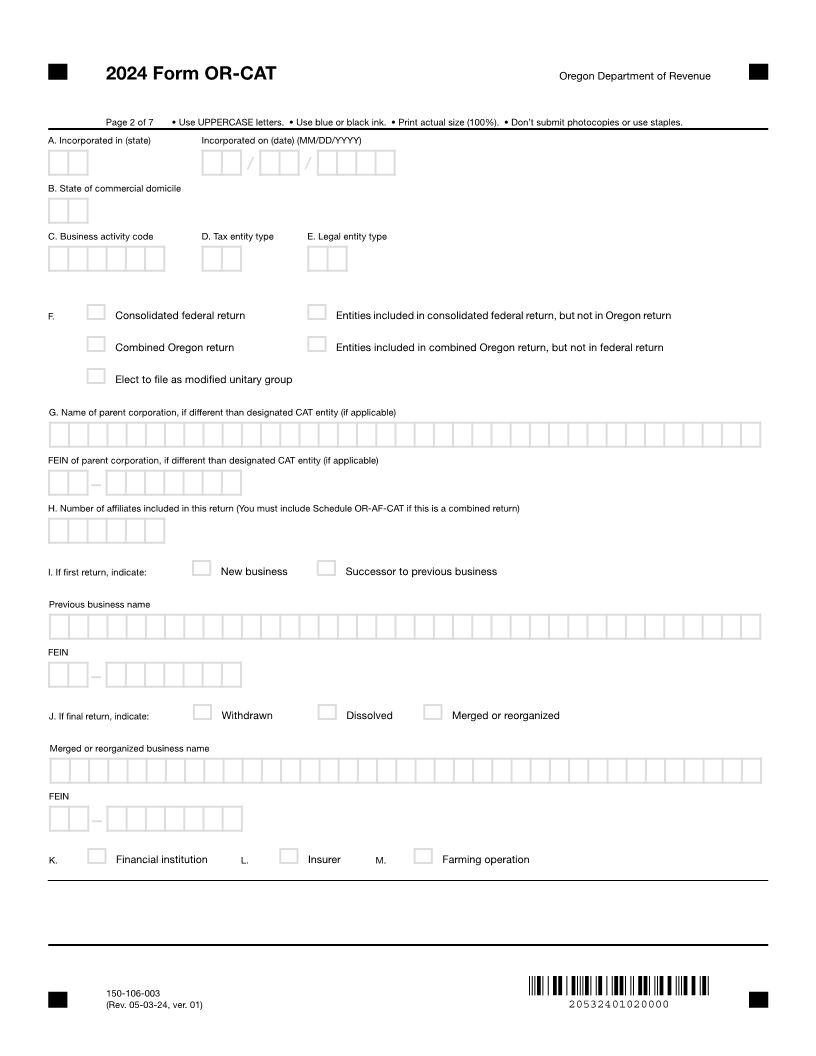
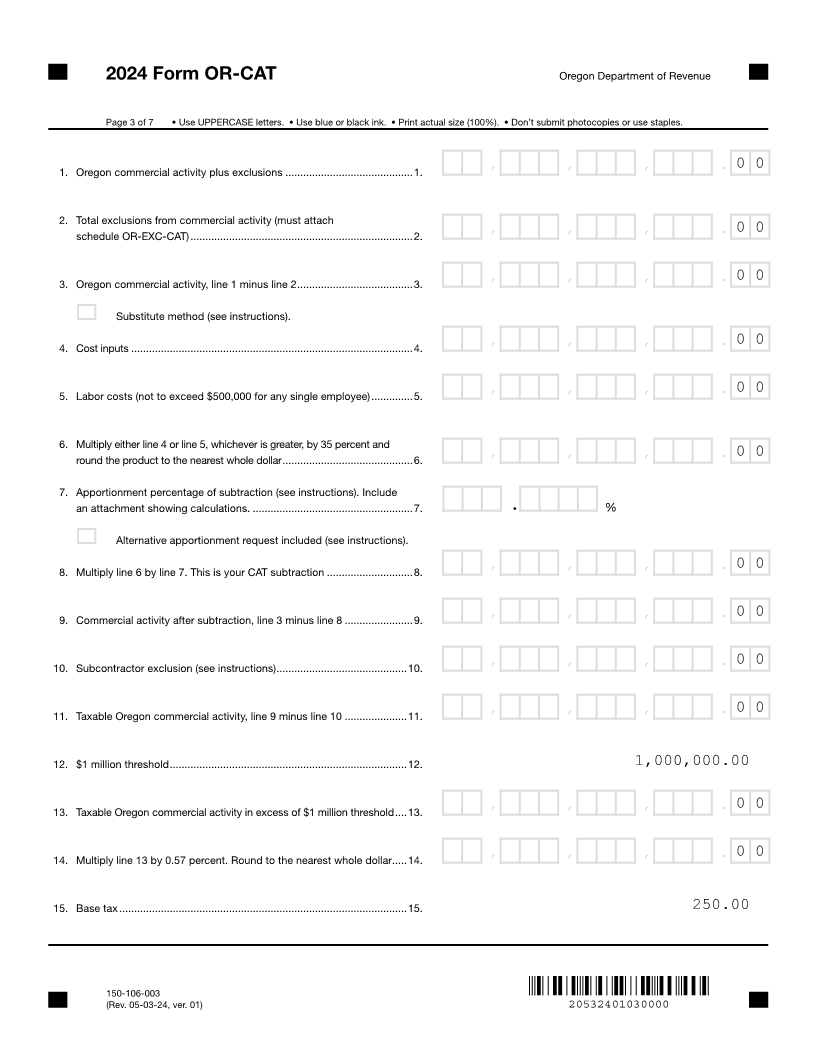
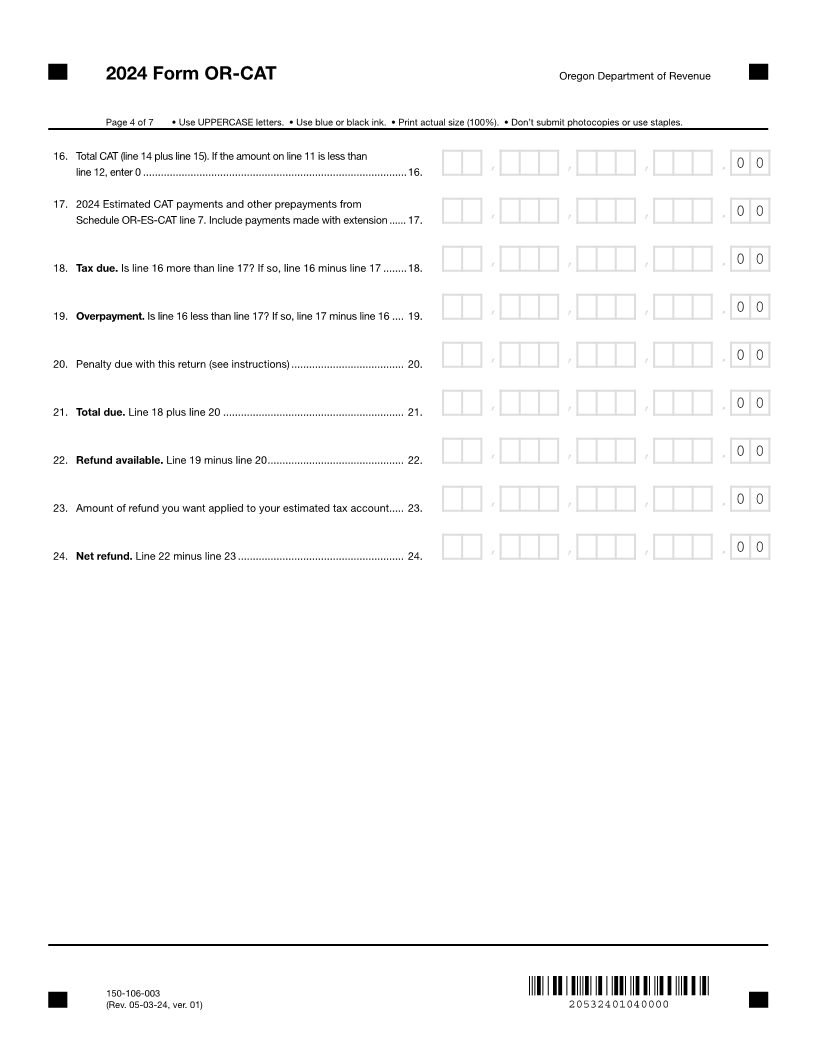
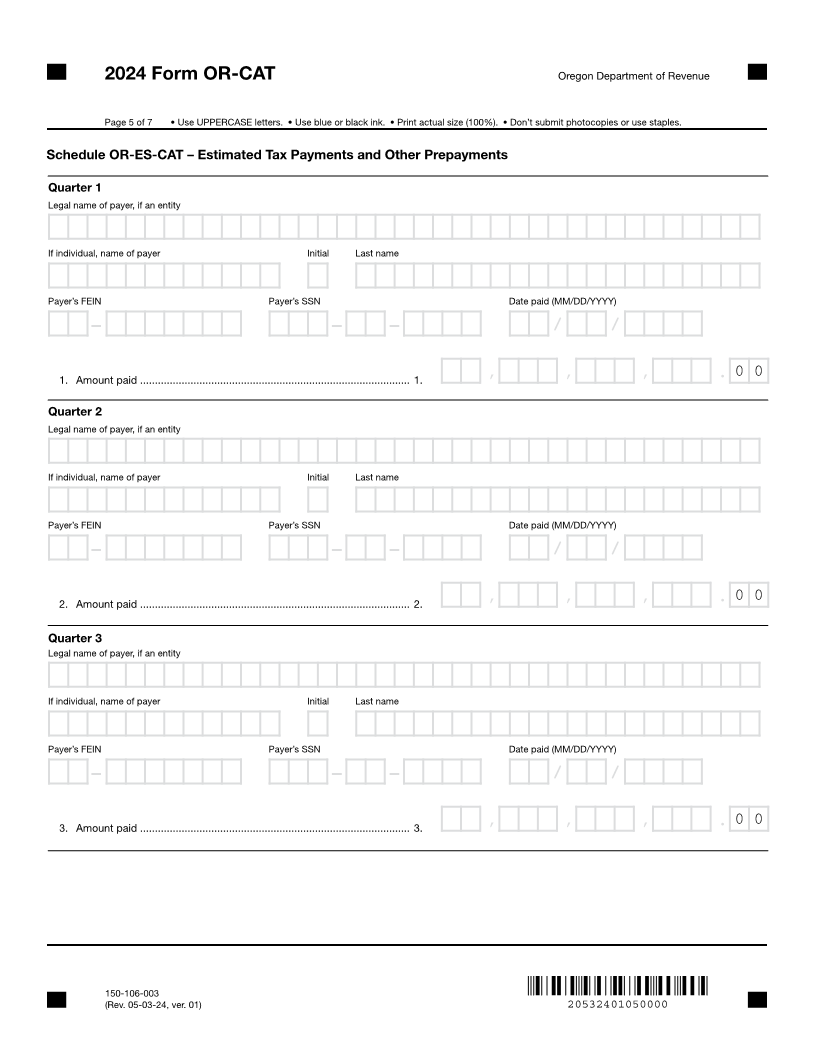
2024 Form OR-CAT
6 Oregon Corporate Activity Tax Return 6
7 7
8 Page 1 of 7 • Use UPPERCASE letters. • Use blue or black ink. • Print actual size (100%). • Don’t submit photocopies or use staples. 8
9 Fiscal year beginning (MM/DD/YYYY) Fiscal year ending (MM/DD/YYYY) 9
10 10
11 99/99/9999/ / 99/99/9999/ / 11
12 12
13 See instructions for checkboxes. 13
14 14
15 X Extension X Amended 15
16 16
17 17
18 X New name X New address X Accounting period change 18
19 19
20 Date beginning (MM/DD/YYYY) Date ending (MM/DD/YYYY) 20
21 X Short-year returns 21
22 99/99/9999/ / 99/99/9999/ / 22
23 23
24 Legal name of designated Corporate Activity Tax (CAT) entity (sole proprietor—complete the next line) 24
25 25
26 26
XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
27 First name (if sole proprietorship) Initial Last name 27
28 28
29 29
XXXXXXXXXXXXXXXX X XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
30 Federal employer identification number (FEIN) Social Security number (SSN) 30
31 31
32 99-9999999 999-99-9999 X Deceased 32
33 Doing business as (DBA) 33
34 34
35 35
XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
36 Current address 36
37 37
38 38
XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
39 City State ZIP code 39
40 40
41 XXXXXXXXXXXXXXXXXXXXXX XX XXXXX-XXXX - 41
42 Country (if other than the U.S.) Contact phone 42
43 43
44 44
XXXXXXXXXXXXXXXXXXXXX 999-999-9999
45 Contact first name Initial Contact last name 45
46 46
47 47
XXXXXXXXXXXXXXXX X XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
48 Email 48
49 49
50 50
XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
51 51
52 52
53 53
54 54
55 55
56 56
57 57
58 58
59 59
60 60
61 61
62 62
150-106-003
63 (Rev. 05-03-24, ver. 01) 20532401010000 63
64 64
1 2 65 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 65 84 85
3 4 82 83
66 66