Enlarge image
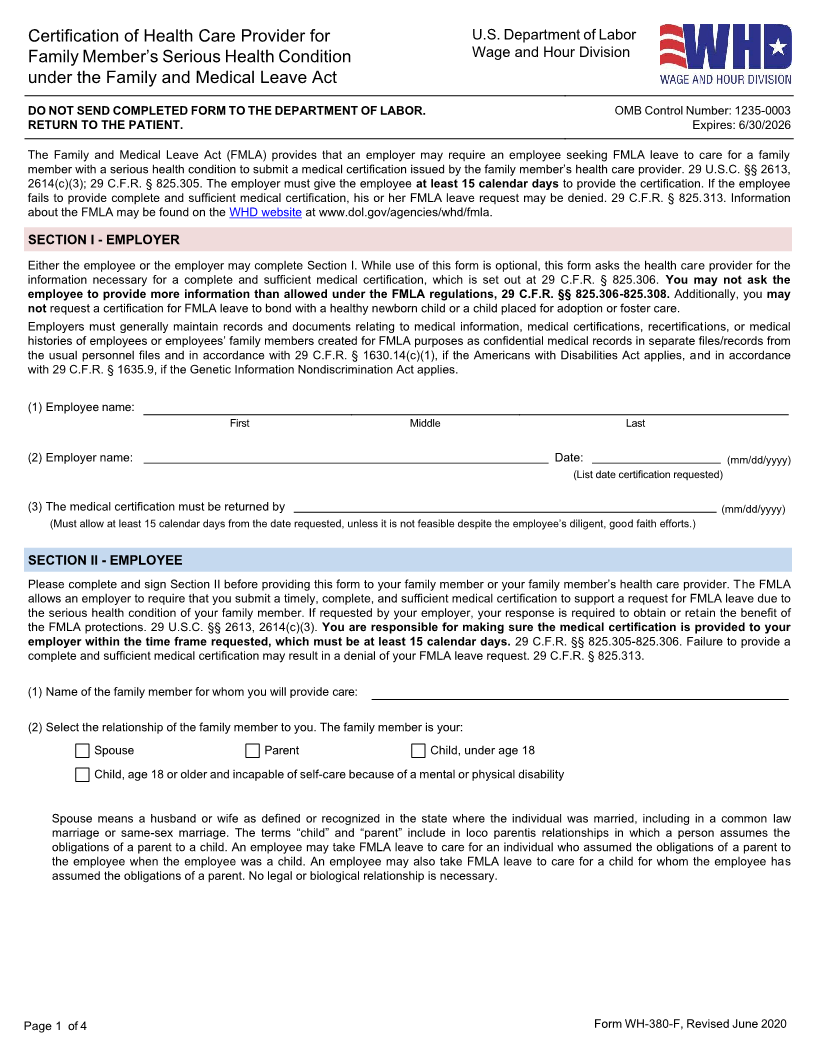
Certification of Health Care Provider for U.S. Department of Labor
Family Member’s Serious Health Condition Wage and Hour Division
under the Family and Medical Leave Act
DO NOT SEND COMPLETED FORM TO THE DEPARTMENT OF LABOR. OMB Control Number: 1235-0003
RETURN TO THE PATIENT. Expires: 6/30/2026
The Family and Medical Leave Act (FMLA) provides that an employer may require an employee seeking FMLA leave to care for a family
member with a serious health condition to submit a medical certification issued by the family member’s health care provider. 29 U.S.C. §§ 2613,
2614(c)(3); 29 C.F.R. § 825.305. The employer must give the employee at least 15 calendar days to provide the certification. If the employee
fails to provide complete and sufficient medical certification, his or her FMLA leave request may be denied. 29 C.F.R. § 825.313. Information
about the FMLA may be found on the WHD website at www.dol.gov/agencies/whd/fmla.
SECTION I - EMPLOYER
Either the employee or the employer may complete Section I. While use of this form is optional, this form asks the health care provider for the
information necessary for a complete and sufficient medical certification, which is set out at 29 C.F.R. § 825.306. You may not ask the
employee to provide more information than allowed under the FMLA regulations, 29 C.F.R. §§ 825.306-825.308. Additionally, you may
not request a certification for FMLA leave to bond with a healthy newborn child or a child placed for adoption or foster care.
Employers must generally maintain records and documents relating to medical information, medical certifications, recertifications, or medical
histories of employees or employees’ family members created for FMLA purposes as confidential medical records in separate files/records from
the usual personnel files and in accordance with 29 C.F.R. § 1630.14(c)(1), if the Americans with Disabilities Act applies, and in accordance
with 29 C.F.R. § 1635.9, if the Genetic Information Nondiscrimination Act applies.
(1) Employee name:
First Middle Last
(2) Employer name: Date: (mm/dd/yyyy)
(List date certification requested)
(3) The medical certification must be returned by (mm/dd/yyyy)
(Must allow at least 15 calendar days from the date requested, unless it is not feasible despite the employee’s diligent, good faith efforts.)
SECTION II - EMPLOYEE
Please complete and sign Section II before providing this form to your family member or your family member’s health care provider. The FMLA
allows an employer to require that you submit a timely, complete, and sufficient medical certification to support a request for FMLA leave due to
the serious health condition of your family member. If requested by your employer, your response is required to obtain or retain the benefit of
the FMLA protections. 29 U.S.C. §§ 2613, 2614(c)(3). You are responsible for making sure the medical certification is provided to your
employer within the time frame requested, which must be at least 15 calendar days. 29 C.F.R. §§ 825.305-825.306. Failure to provide a
complete and sufficient medical certification may result in a denial of your FMLA leave request. 29 C.F.R. § 825.313.
(1) Name of the family member for whom you will provide care:
(2) Select the relationship of the family member to you. The family member is your:
Spouse Parent Child, under age 18
Child, age 18 or older and incapable of self-care because of a mental or physical disability
Spouse means a husband or wife as defined or recognized in the state where the individual was married, including in a common law
marriage or same-sex marriage. The terms “child” and “parent” include in loco parentis relationships in which a person assumes the
obligations of a parent to a child. An employee may take FMLA leave to care for an individual who assumed the obligations of a parent to
the employee when the employee was a child. An employee may also take FMLA leave to care for a child for whom the employee has
assumed the obligations of a parent. No legal or biological relationship is necessary.
Page 1 of 4 Form WH-380-F, Revised June 2020