- 3 -
Enlarge image
|
RPD-41206
Rev. 02/27/2024 New Mexico Taxation and Revenue Department
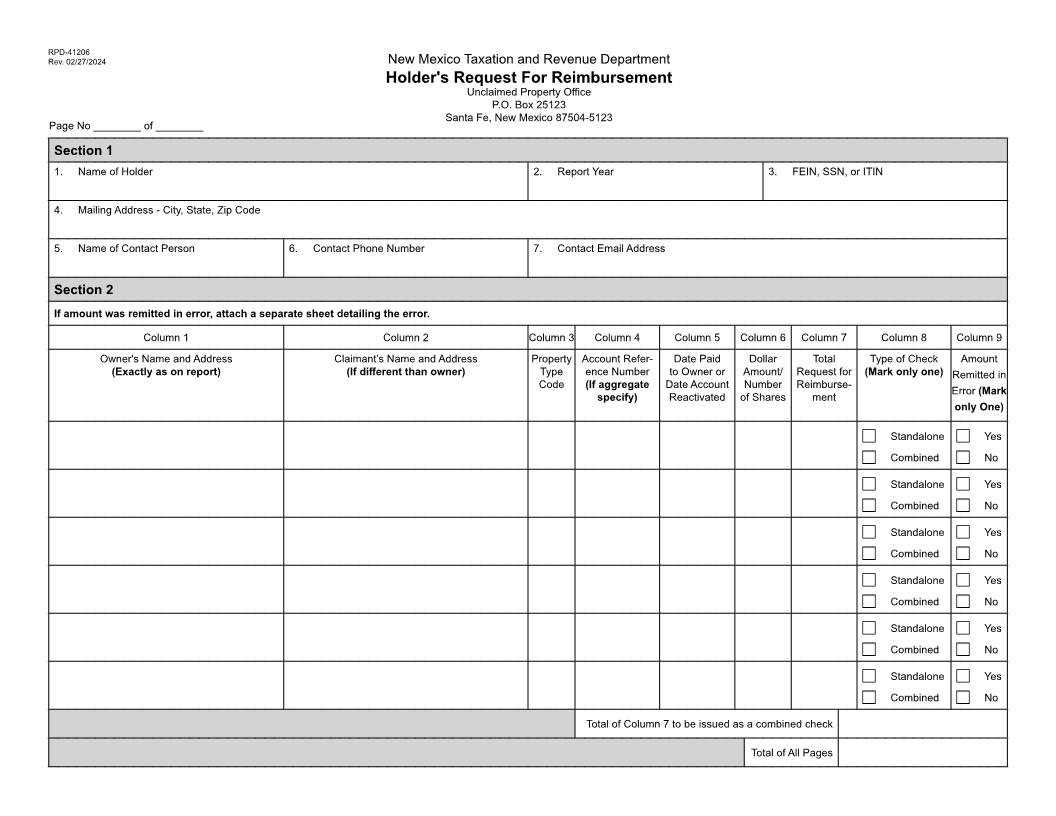
Holder's Request For Reimbursement
Instructions
This form is used to request a reimbursement, or refund, or Period and Property Type Codes Schedule. The
both for amounts that were submitted in error or amounts that number to the right of the property type indicates
have been paid to the owner by holder. the number of years of inactivity after which the
account should be reported as unclaimed.
In the reimbursement process, a holder decides to pay an Column 4: Account Reference Number
owner and then files a claim with the Unclaimed Property Enter account reference number. If aggregate-
Office (UPO) for reimbursement. We encourage the holder specify.
to use the reimbursement process for those customers and Column 5: Date Paid to Owner or Date Account Reacti-
owners demanding immediate payment or reinstatement of vated
their accounts. The UPO makes every effort to respond to Enter the date that the amount was paid to owner
your request as quickly as possible. or the date the account was reactivated.
Column 6: Dollar Amount/Number of Shares
Refunds are made to holders who have overpaid their un- Enter the dollar amount and/or the number of
claimed property reports. The overpayments are usually shares.
due to accounting errors or other mistakes made during the Column 7: Total Request for Reimbursement
preparation of reports. Enter the total amount of reimbursement for row.
Column 8: Type of Check
Page Number Pages should be numbered consecutively Mark only one box in this column for each row. If
(e.g., page 1 of 24; 2 of 24) at the top of the form. Page holder is requesting a single check for the amount
totals of amounts for a combined check, column 7 are to be in row mark Standalone. If holder is requesting
entered on each page and the grand total should be entered a combined check for multiple rows mark Com-
on the last page. bined, then total at the bottom of the page.
Column 8: Amount Remitted in Error
FORM INSTRUCTIONS Mark only one box in this columns for each row.
If the amount was remitted in error mark yes and
Section 1 attach a separate sheet detailing the error. If the
1. Name of Holder amount was not remitted in error mark no.
Enter the name of the holder.
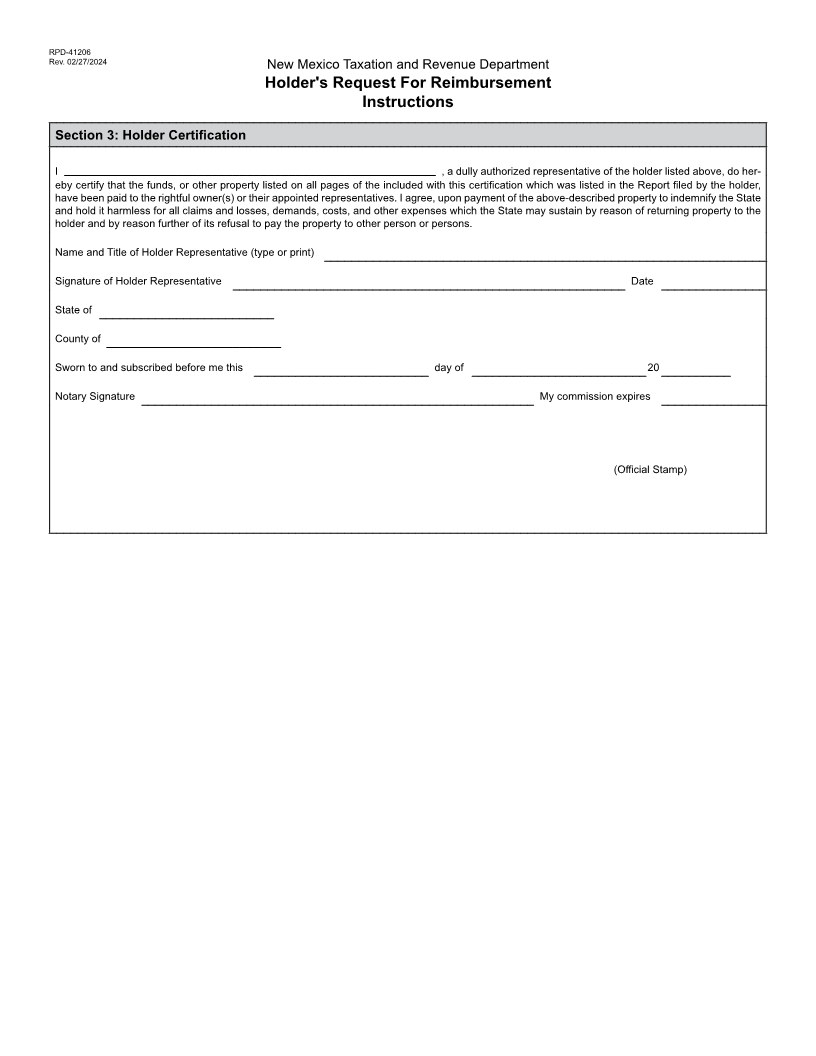
2. Report Year Section 3
Enter the report year applicable to this report. Complete this section of the form which is a sworn statement
3. FEIN, SSN, or ITIN by the holder or holders representative indicating that the
Enter the FEIN, SSN, or ITIN of the holder. statement is accurate, and that all other information provided
4. Mailing Address - City, State, Zip Code in the report is true and correct to the best of the holders' or
Enter the mailing address of the holder. holder's representative's knowledge.
5. Name of Contact Person
Enter contact person's name. You may photocopy this form as needed.
6. Contact Phone Number
Enter contact person's phone number. If you have any questions please contact the Unclaimed
7. Contact Email Property Office at:
Enter contact person's email address.
New Mexico Taxation & Revenue Department
Section 2 Unclaimed Property Office
Column 1: Owner's Name and Address P.O. Box 25123
List alphabetically. Enter owner’s last name, first Santa Fe, New Mexico 87504-5123
name, middle name or initial; and address. Use Unclaimed.Property@tax.nm.gov
one block for each owner’s name and address. If 505-827-0668
there is joint ownership of the securities, list both
names within the same block.
Column 2: Claimant’s Name and Address
If claimant is different than owner enter claimant's
last name, first name, middle name or initial; and
address;
Column 3: Property Type Code
Enter the proper property type code correspond-
ing to the description as listed on the Retention
|