Enlarge image
RPD-41206
Rev. 02/27/2024 New Mexico Taxation and Revenue Department
Holder's Request For Reimbursement
Unclaimed Property Office
P.O. Box 25123
Santa Fe, New Mexico 87504-5123
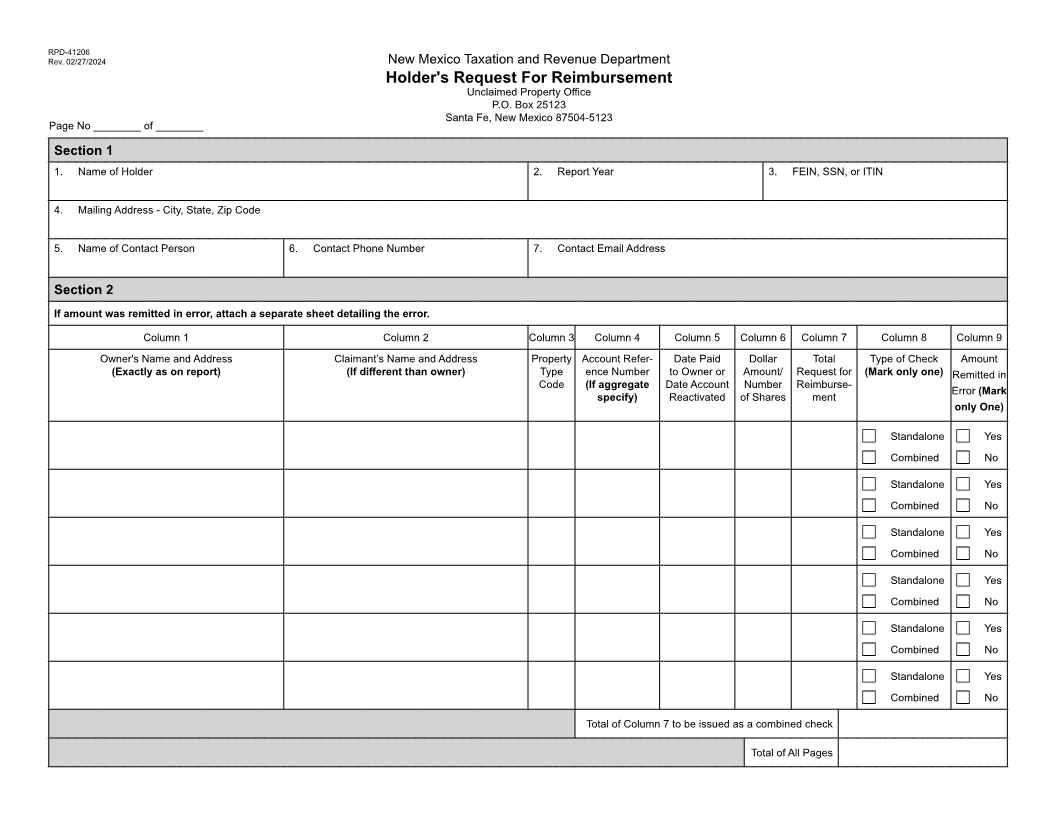
Page No ________ of ________
Section 1
1. Name of Holder 2. Report Year 3. FEIN, SSN, or ITIN
4. Mailing Address - City, State, Zip Code
5. Name of Contact Person 6. Contact Phone Number 7. Contact Email Address
Section 2
If amount was remitted in error, attach a separate sheet detailing the error.
Column 1 Column 2 Column 3 Column 4 Column 5 Column 6 Column 7 Column 8 Column 9
Owner's Name and Address Claimant’s Name and Address Property Account Refer- Date Paid Dollar Total Type of Check Amount
(Exactly as on report) (If different than owner) Type ence Number to Owner or Amount/ Request for (Mark only one) Remitted in
Code (If aggregate Date Account Number Reimburse- Error (Mark
specify) Reactivated of Shares ment
only One)
c Standalone c Yes
c Combined c No
c Standalone c Yes
c Combined c No
c Standalone c Yes
c Combined c No
c Standalone c Yes
c Combined c No
c Standalone c Yes
c Combined c No
c Standalone c Yes
c Combined c No
Total of Column 7 to be issued as a combined check
Total of All Pages