Enlarge image
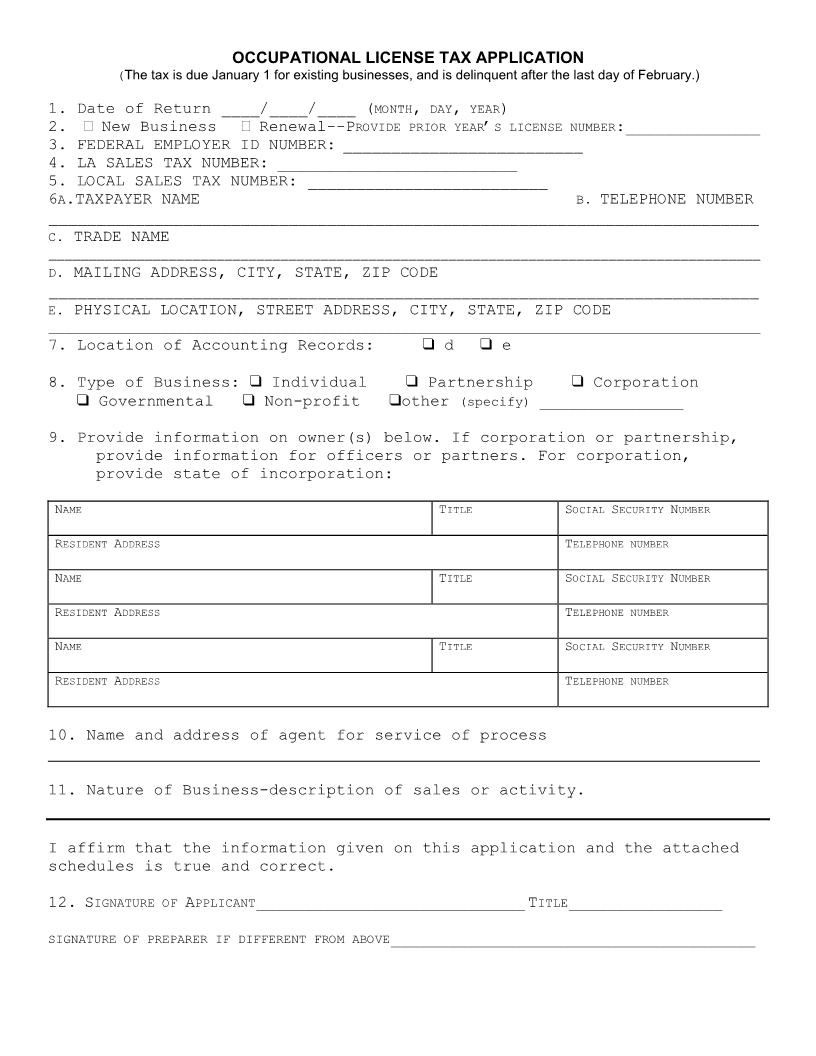
OCCUPATIONAL LICENSE TAX APPLICATION
(The tax is due January 1 for existing businesses, and is delinquent after the last day of February.)
1. Date of Return ____/____/____ (MONTH ,DAY ,YEAR)
2. New Business Renewal--PROVIDE PRIOR YEAR’S LICENSE NUMBER:______________
3. FEDERAL EMPLOYER ID NUMBER: _________________________
4. LA SALES TAX NUMBER: _________________________
5. LOCAL SALES TAX NUMBER: _________________________
6A.TAXPAYER NAME B.TELEPHONE NUMBER
__________________________________________________________________________
C. TRADE NAME
_________________________________________________________________________________________
D. MAILING ADDRESS, CITY, STATE, ZIP CODE
__________________________________________________________________________
E. PHYSICAL LOCATION, STREET ADDRESS, CITY, STATE, ZIP CODE
_________________________________________________________________________________________
7. Location of Accounting Records: “ d “ e
8. Type of Business: “ Individual “ Partnership “Corporation
“ Governmental “ Non-profit “ other (specify)_______________
9. Provide information on owner(s) below. If corporation or partnership,
provide information for officers or partners. For corporation,
provide state of incorporation:
NAME TITLE SOCIAL SECURITY NUMBER
RESIDENT ADDRESS TELEPHONE NUMBER
NAME TITLE SOCIAL SECURITY NUMBER
RESIDENT ADDRESS TELEPHONE NUMBER
NAME TITLE SOCIAL SECURITY NUMBER
RESIDENT ADDRESS TELEPHONE NUMBER
10. Name and address of agent for service of process
________________________________________________________________________________
11. Nature of Business-description of sales or activity.
I affirm that the information given on this application and the attached
schedules is true and correct.
12. SIGNATURE OF APPLICANT____________________________ TITLE________________
SIGNATURE OF PREPARER IF DIFFERENT FROM ABOVE______________________________________