Enlarge image
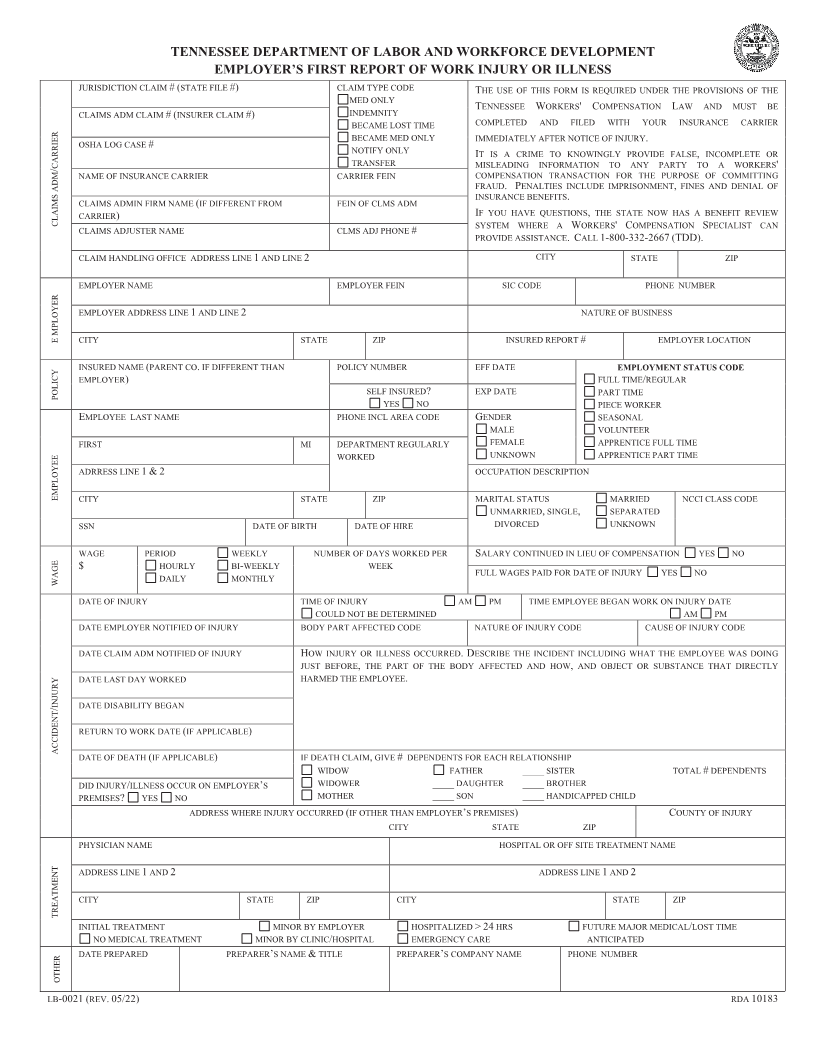
TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT
EMPLOYER’S FIRST REPORT OF WORK INJURY OR ILLNESS
JURISDICTION CLAIM #(STATE FILE #) CLAIM TYPE CODE THE USE OF THIS FORM IS REQUIRED UNDER THE PROVISIONS OF THE
MED ONLY
CLAIMS ADM CLAIM #(INSURER CLAIM #) INDEMNITY TENNESSEE WORKERS'COMPENSATION LAW AND MUST BE
BECAME LOST TIME COMPLETED AND FILED WITH YOUR INSURANCE CARRIER
BECAME MED ONLY IMMEDIATELY AFTER NOTICE OF INJURY.
OSHA LOG CASE # NOTIFY ONLY IT IS A CRIME TO KNOWINGLY PROVIDE FALSE INCOMPLETE, OR
CARRIER/ TRANSFER MISLEADING INFORMATION TO ANY PARTY TO A WORKERS'
NAME OF INSURANCE CARRIER CARRIER FEIN COMPENSATION TRANSACTION FOR THE PURPOSE OF COMMITTING
FRAUD.PENALTIES INCLUDE IMPRISONMENT ,FINES AND DENIAL OF
INSURANCE BENEFITS
CLAIMS ADMIN FIRM NAME (IF DIFFERENT FROM FEIN OF CLMS ADM .
CARRIER) IF YOU HAVE QUESTIONS THE,STATE NOW HAS A BENEFIT REVIEW
CLAIMS ADM CLAIMS ADJUSTER NAME CLMS ADJ PHONE # SYSTEM WHERE A WORKERS'COMPENSATION SPECIALIST CAN
PROVIDE ASSISTANCE.CALL 1-800-332-2667 (TDD).
CLAIM HANDLING OFFICE ADDRESS LINE 1AND LINE 2 CITY STATE ZIP
EMPLOYER NAME EMPLOYER FEIN SIC CODE PHONE NUMBER
EMPLOYER ADDRESS LINE 1AND LINE 2 NATURE OF BUSINESS
E MPLOYER CITY STATE ZIP INSURED REPORT # EMPLOYER LOCATION
INSURED NAME (PARENT CO .IF DIFFERENT THAN POLICY NUMBER EFF DATE EMPLOYMENT STATUS CODE
EMPLOYER) FULL TIME/REGULAR
POLICY SELF INSURED? EXP DATE PART TIME
YES NO PIECE WORKER
EMPLOYEE LAST NAME PHONE INCL AREA CODE GENDER SEASONAL
MALE VOLUNTEER
FIRST MI DEPARTMENT REGULARLY FEMALE APPRENTICE FULL TIME
WORKED UNKNOWN APPRENTICE PART TIME
ADRRESS LINE 1& 2 OCCUPATION DESCRIPTION
EMPLOYEE CITY STATE ZIP MARITAL STATUS MARRIED NCCI CLASS CODE
UNMARRIED ,SINGLE, SEPARATED
SSN DATE OF BIRTH DATE OF HIRE DIVORCED UNKNOWN
WAGE PERIOD WEEKLY NUMBER OF DAYS WORKED PER SALARY CONTINUED IN LIEU OF COMPENSATION YES NO
$ HOURLY BI-WEEKLY WEEK
WAGE DAILY MONTHLY FULL WAGES PAID FOR DATE OF INJURY YES NO
DATE OF INJURY TIME OF INJURY AM PM TIME EMPLOYEE BEGAN WORK ON INJURY DATE
COULD NOT BE DETERMINED AM PM
DATE EMPLOYER NOTIFIED OF INJURY BODY PART AFFECTED CODE NATURE OF INJURY CODE CAUSE OF INJURY CODE
DATE CLAIM ADM NOTIFIED OF INJURY HOW INJURY OR ILLNESS OCCURRED.DESCRIBE THE INCIDENT INCLUDING WHAT THE EMPLOYEE WAS DOING
JUST BEFORE ,THE PART OF THE BODY AFFECTED AND HOW AND,OBJECT OR SUBSTANCE THAT DIRECTLY
DATE LAST DAY WORKED HARMED THE EMPLOYEE.
INJURY/ DATE DISABILITY BEGAN
RETURN TO WORK DATE (IF APPLICABLE )
ACCIDENT
DATE OF DEATH (IF APPLICABLE) IF DEATH CLAIM ,GIVE #DEPENDENTS FOR EACH RELATIONSHIP
WIDOW FATHER ____SISTER TOTAL #DEPENDENTS
DID INJURY/ILLNESS OCCUR ON EMPLOYER’S WIDOWER ____DAUGHTER ____BROTHER
PREMISES? YES NO MOTHER ____ SON ____ HANDICAPPED CHILD
ADDRESS WHERE INJURY OCCURRED (IF OTHER THAN EMPLOYER’S PREMISES ) C OUNTY OF INJURY
CITY STATE ZIP
PHYSICIAN NAME HOSPITAL OR OFF SITE TREATMENT NAME
ADDRESS LINE 1AND 2 ADDRESS LINE 1AND 2
CITY STATE ZIP CITY STATE ZIP
TREATMENT
INITIAL TREATMENT MINOR BY EMPLOYER HOSPITALIZED>24 HRS FUTURE MAJOR MEDICAL/LOST TIME
NO MEDICAL TREATMENT MINOR BY CLINIC/HOSPITAL EMERGENCY CARE ANTICIPATED
DATE PREPARED PREPARER’S NAME &TITLE PREPARER’S COMPANY NAME PHONE NUMBER
OTHER
LB-0021 (REV. 05/22) RDA10183