Enlarge image
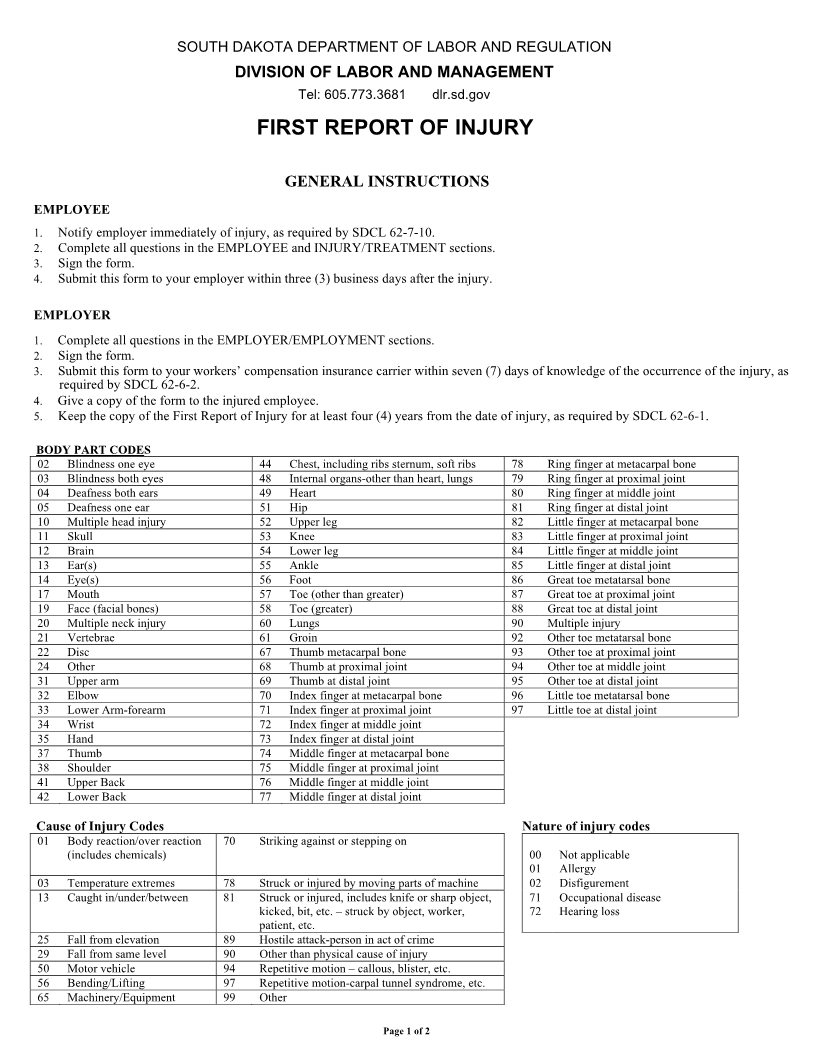
SOUTH DAKOTA DEPARTMENT OF LABOR AND REGULATION
DIVISION OF LABOR AND MANAGEMENT
Tel: 605.773.3681 dlr.sd.gov
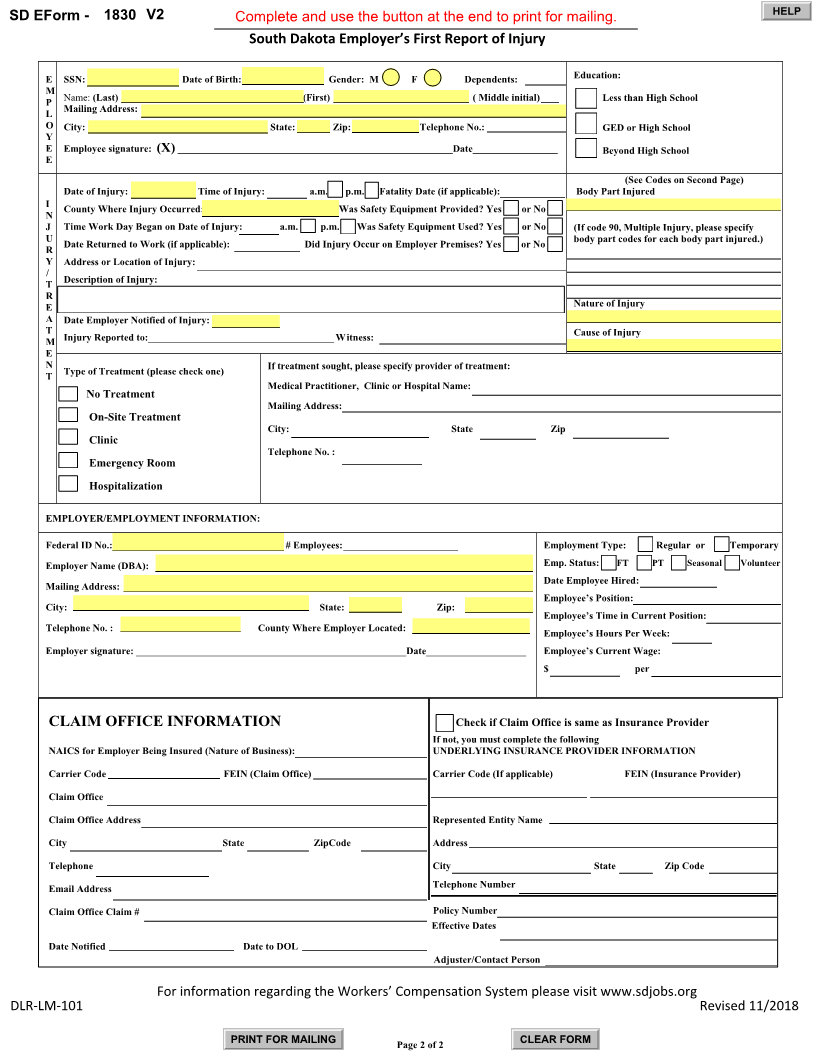
FIRST REPORT OF INJURY
GENERAL INSTRUCTIONS
EMPLOYEE
1. Notify employer immediately of injury, as required by SDCL 62-7-10.
2. Complete all questions in the EMPLOYEE and INJURY/TREATMENT sections.
3. Sign the form.
4. Submit this form to your employer within three (3) business days after the injury.
EMPLOYER
1. Complete all questions in the EMPLOYER/EMPLOYMENT sections.
2. Sign the form.
3. Submit this form to your workers’ compensation insurance carrier within seven (7) days of knowledge of the occurrence of the injury, as
required by SDCL 62-6-2.
4. Give a copy of the form to the injured employee.
5. Keep the copy of the First Report of Injury for at least four (4) years from the date of injury, as required by SDCL 62-6-1.
BODY PART CODES
02 Blindness one eye 44 Chest, including ribs sternum, soft ribs 78 Ring finger at metacarpal bone
03 Blindness both eyes 48 Internal organs-other than heart, lungs 79 Ring finger at proximal joint
04 Deafness both ears 49 Heart 80 Ring finger at middle joint
05 Deafness one ear 51 Hip 81 Ring finger at distal joint
10 Multiple head injury 52 Upper leg 82 Little finger at metacarpal bone
11 Skull 53 Knee 83 Little finger at proximal joint
12 Brain 54 Lower leg 84 Little finger at middle joint
13 Ear(s) 55 Ankle 85 Little finger at distal joint
14 Eye(s) 56 Foot 86 Great toe metatarsal bone
17 Mouth 57 Toe (other than greater) 87 Great toe at proximal joint
19 Face (facial bones) 58 Toe (greater) 88 Great toe at distal joint
20 Multiple neck injury 60 Lungs 90 Multiple injury
21 Vertebrae 61 Groin 92 Other toe metatarsal bone
22 Disc 67 Thumb metacarpal bone 93 Other toe at proximal joint
24 Other 68 Thumb at proximal joint 94 Other toe at middle joint
31 Upper arm 69 Thumb at distal joint 95 Other toe at distal joint
32 Elbow 70 Index finger at metacarpal bone 96 Little toe metatarsal bone
33 Lower Arm-forearm 71 Index finger at proximal joint 97 Little toe at distal joint
34 Wrist 72 Index finger at middle joint
35 Hand 73 Index finger at distal joint
37 Thumb 74 Middle finger at metacarpal bone
38 Shoulder 75 Middle finger at proximal joint
41 Upper Back 76 Middle finger at middle joint
42 Lower Back 77 Middle finger at distal joint
Cause of Injury Codes Nature of injury codes
01 Body reaction/over reaction 70 Striking against or stepping on
(includes chemicals) 00 Not applicable
01 Allergy
03 Temperature extremes 78 Struck or injured by moving parts of machine 02 Disfigurement
13 Caught in/under/between 81 Struck or injured, includes knife or sharp object, 71 Occupational disease
kicked, bit, etc. – struck by object, worker, 72 Hearing loss
patient, etc.
25 Fall from elevation 89 Hostile attack-person in act of crime
29 Fall from same level 90 Other than physical cause of injury
50 Motor vehicle 94 Repetitive motion – callous, blister, etc.
56 Bending/Lifting 97 Repetitive motion-carpal tunnel syndrome, etc.
65 Machinery/Equipment 99 Other
Page 1 of 2