Enlarge image
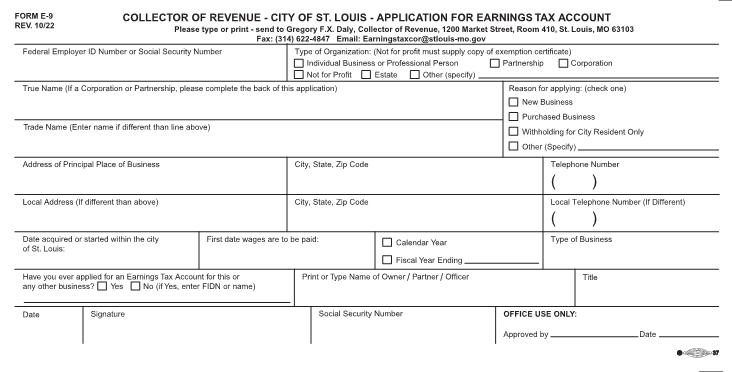
FORM E-9 COLLECTOR OF REVENUE - CITY OF ST. LOUIS - APPLICATION FOR EARNINGS TAX ACCOUNT REV. 10/22 Please type or print - send to Gregory F.X. Daly, Collector of Revenue, 1200 Market Street, Room 410, St. Louis, MO 63103 Fax: (314) 622-4847 Email: Earningstaxcor@stlouis-mo.gov Federal Employer ID Number or Social Security Number Type of Organization: (Not for profit must supply copy of exemption certificate) Individual Business or Professional Person Partnership Corporation Not for Profit Estate Other (specify) True Name (If a Corporation or Partnership, please complete the back of this application) Reason for applying: (check one) New Business Purchased Business Trade Name (Enter name if different than line above) Withholding for City Resident Only Other (Specify) Address of Principal Place of Business City, State, Zip Code Telephone Number ( ) Local Address (If different than above) City, State, Zip Code Local Telephone Number (If Different) ( ) Date acquired or started within the city First date wages are to be paid: Calendar Year Type of Business of St. Louis: Fiscal Year Ending Have you ever applied for an Earnings Tax Account for this or Print or Type Name of Owner /Partner /Officer Title any other business? Yes No (if Yes, enter FIDN or name) Date Signature Social Security Number OFFICE USE ONLY: Approved by Date