Enlarge image
REQUIREMENTS FOR MAGNETIC MEDIA REPORTING
of
QUARTERLY PAYROLL REPORT
1. Conform to all technical specifications (see Appendix A). Also refer to specifications outlined
in the U.S. Department of Health and Human Services publication Magnetic Media Reporting.
2. If this is your first magnetic filing, submit a hard copy of your wage data with your media (CD-R,
cartridge ). If the media is correct, it will be processed. If it is rejected, the hard copy will be
processed and we will notify you of the problems. After you receive notification that you are an
approved magnetic media reporter, it is no longer necessary to provide a hard copy.
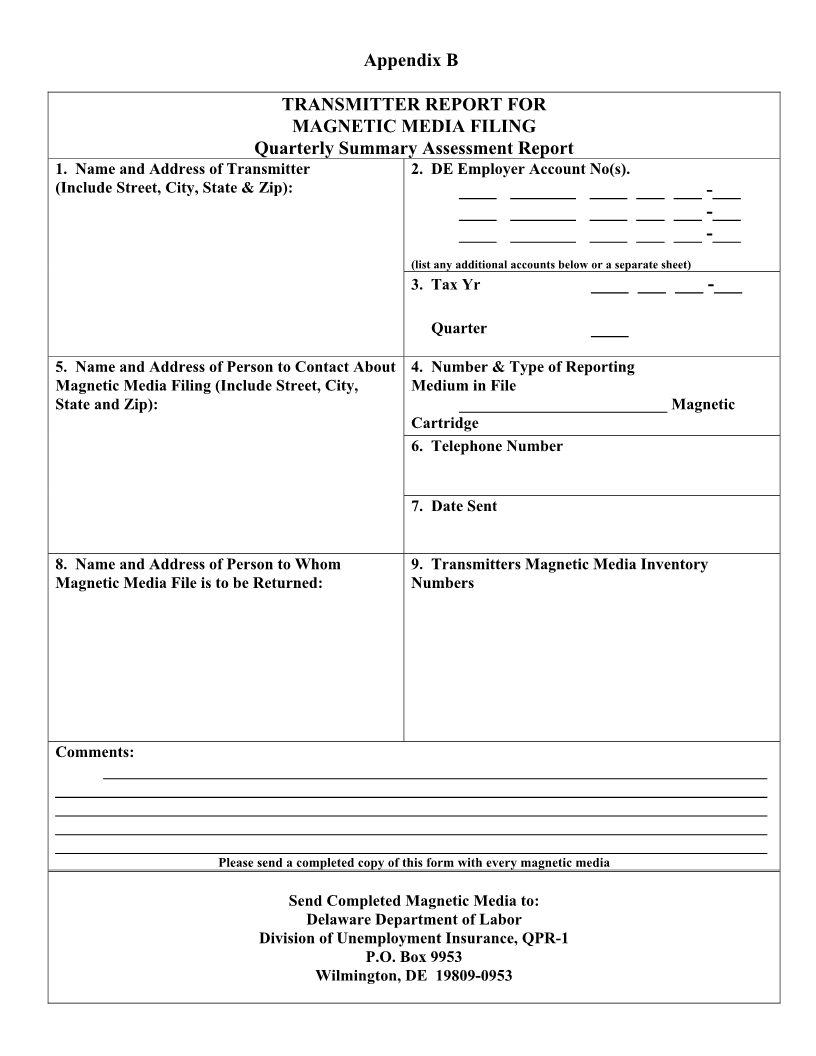
3. Include a copy of a completed Transmitter Report with each media . (see Appendix B).
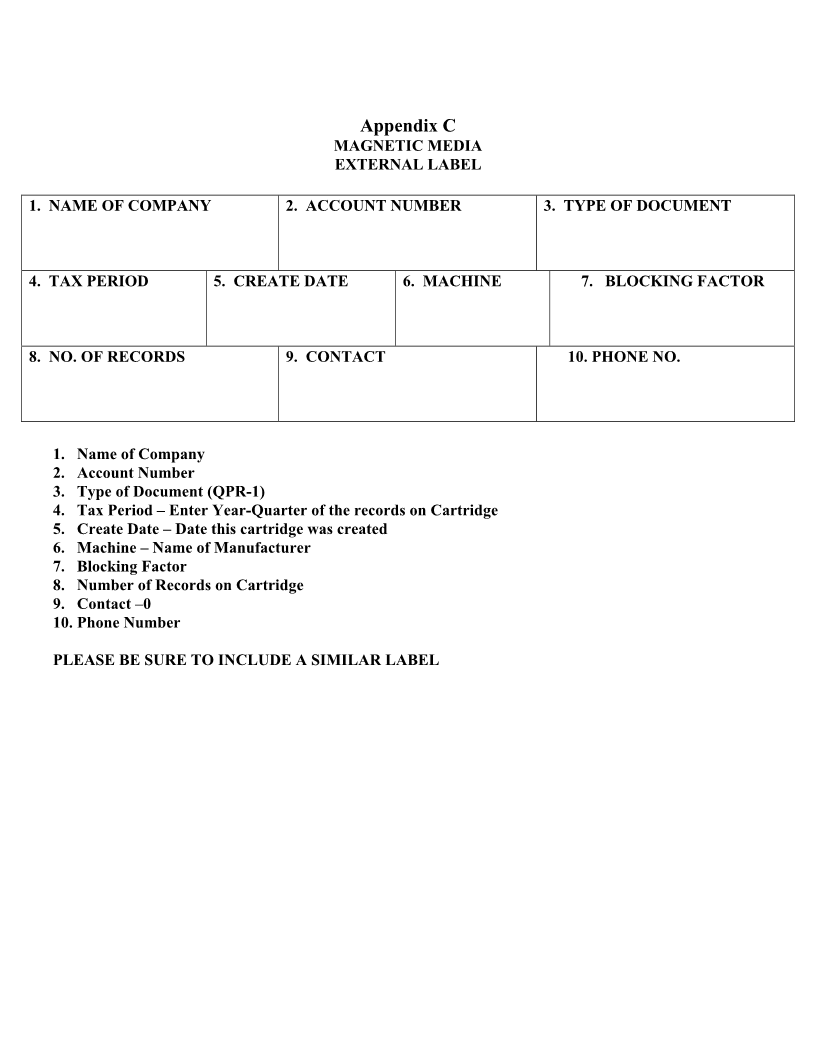
4. If you are using a CD-R -use a felt tip permanent marker to label the CD-R, place the CD-R in a
protective case and place an external label on the outside of the protective case that includes all
necessary information. (see Appendix C).
For cartridges place an external label on each cartridge that includes all necessary information. (see
Appendix C).
5. Please give each CD-R /cartridge an external catalogue number or some other identification number
(any length).
6. Send the magnetic media to the following address: Delaware Department of Labor
Div. of Unemployment Insurance
P. O. Box 9953
Wilmington, DE 19809
7. Send the Quarterly Tax Report (DE form UC-8) and Quarterly Payroll Report (DE form UC-8A) with
the notation filed by magnetic media to: Delaware Department of Labor
Div. of Unemployment Insurance
P. O. Box 41785
Philadelphia, PA 19101-1785
8. Direct questions to Accounts Management at (302) 761-8482 or at the Delaware address above.