Enlarge image
MARK CHURCH
EF-267-H-R08-0611-41000806-1 Assessor - County Clerk - Recorder
BOE-267-H (P1) REV. 08 (06-11) 555 County Center
WELFARE EXEMPTION SUPPLEMENTAL AFFIDAVIT, Redwood City, CA 94063
P 650.363.4500 F 650.599.7435
HOUSING – ELDERLY OR HANDICAPPED FAMILIES email assessor@smcacre.org
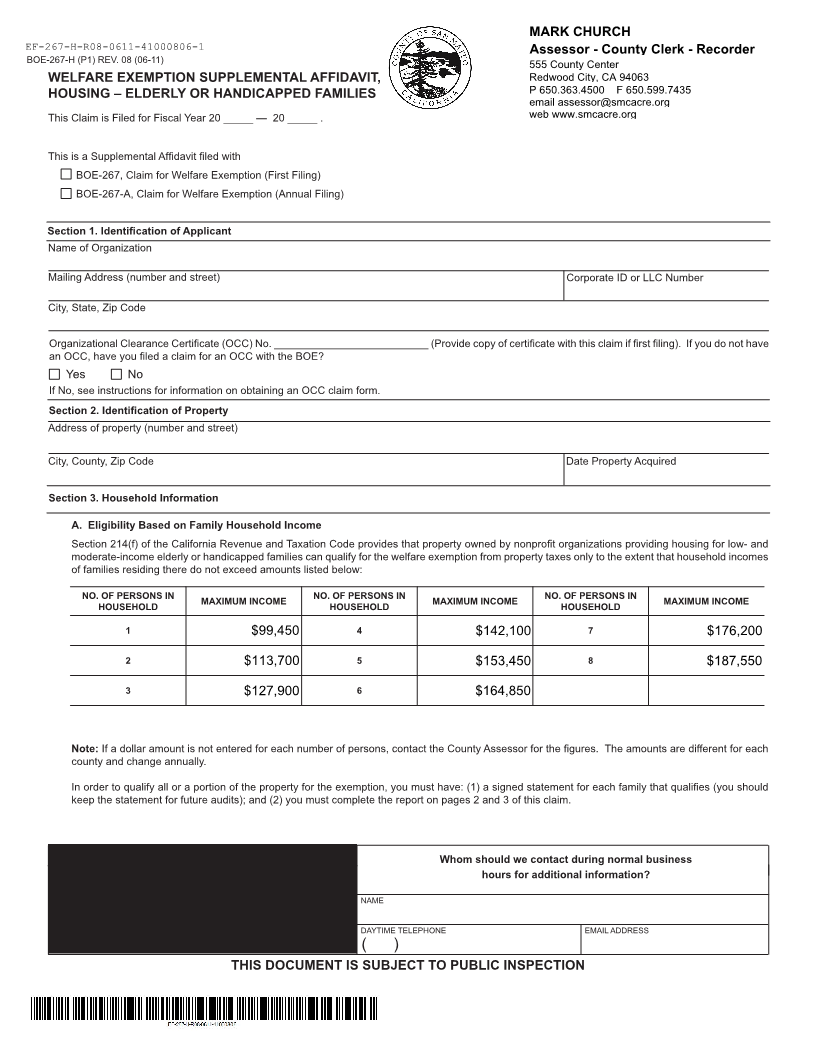
This Claim is Filed for Fiscal Year 20 _____ — 20 _____ . web www.smcacre.org
This is a Supplemental Affidavit filed with
BOE-267, Claim for Welfare Exemption (First Filing)
BOE-267-A, Claim for Welfare Exemption (Annual Filing)
Section 1. Identification of Applicant
Name of Organization
Mailing Address (number and street) Corporate ID or LLC Number
City, State, Zip Code
Organizational Clearance Certificate (OCC) No. __________________________ (Provide copy of certificate with this claim if first filing). If you do not have
an OCC, have you filed a claim for an OCC with the BOE?
Yes No
If No, see instructions for information on obtaining an OCC claim form.
Section 2. Identification of Property
Address of property (number and street)
City, County, Zip Code Date Property Acquired
Section 3. Household Information
A. Eligibility Based on Family Household Income
Section 214(f) of the California Revenue and Taxation Code provides that property owned by nonprofit organizations providing housing for low- and
moderate-income elderly or handicapped families can qualify for the welfare exemption from property taxes only to the extent that household incomes
of families residing there do not exceed amounts listed below:
NO. OF PERSONS IN MAXIMUM INCOME NO. OF PERSONS IN MAXIMUM INCOME NO. OF PERSONS IN MAXIMUM INCOME
HOUSEHOLD HOUSEHOLD HOUSEHOLD
1 $99,450 4 $142,100 7 $176,200
2 $113,700 5 $153,450 8 $187,550
3 $127,900 6 $164,850
Note: If a dollar amount is not entered for each number of persons, contact the County Assessor for the figures. The amounts are different for each
county and change annually.
In order to qualify all or a portion of the property for the exemption, you must have: (1) a signed statement for each family that qualifies (you should
keep the statement for future audits); and (2) you must complete the report on pages 2 and 3 of this claim.
FOR ASSESSOR’S USE ONLY Whom should we contact during normal business
hours for additional information?
Received by (Assessor’s designee) NAME
of (county or city) on (date) DAYTIME TELEPHONE EMAIL ADDRESS
( )
THIS DOCUMENT IS SUBJECT TO PUBLIC INSPECTION