Enlarge image
Arizona Form
Credit for New Employment 2021
345
Include with your return.
For the calendar year 2021 or fiscal year beginning M M D D 2 0 2 1 and ending M M D D Y Y Y Y .
Name as shown on Form 140, 140PY, 140NR, 140X, 140-SBI, 140PY-SBI, 140NR-SBI, 140X-SBI, Social Security or
99T, 120, 120A, 120S, 120X, or 165 Employer Identification Number
Part 1 Business Information
1 Business Name
2 Business Location Address — Street
City State ZIP Code
3 Employer Identification Number
4a What type of entity is the business?
C Corporation Exempt Organization Limited Liability Company (LLC)
Partnership S Corporation Sole Proprietorship
4b If the business is an LLC, what is the federal tax classification? Check only one box:
C Corporation Disregarded Entity Partnership S Corporation
If the business is an LLC, a partnership or an S Corporation, include a schedule that lists ownership information including: name, address, TIN,
and ownership percentage at the end of the tax year.
Part 2 Qualification for Credit
5 Did you receive certification from the Arizona Commerce Authority? .......................................... Yes No
If “Yes”, include a copy of the Certification.
6 Are you claiming a pass through of this credit from a partnership and/or an S Corporation? ..... Yes No
If “Yes”, include a copy of Form(s) 345-P and/or Form(s) 345-S.
7 If you answered “Yes” to the question on line 5 or on line 6, go to Part 3.
If you answered “No” to the questions on line 5 and on line 6, STOP!
YOU ARE NOT ELIGIBLE TO CLAIM THIS CREDIT.
Part 3 Current Taxable Year’s Credit Calculation
(a) (b)
Number of Available Credit:
Employees
Multiply column (a) by $3,000.
8 Credit for employees in first year or partial year of employment in a qualified employment
position ................................................................................................................................. 8 00
9 Credit for employees in the second year of continuous employment in a qualified
employment position............................................................................................................. 9 00
10 Credit for employees in the third year of continuous employment in a qualified
employment position............................................................................................................. 10 00
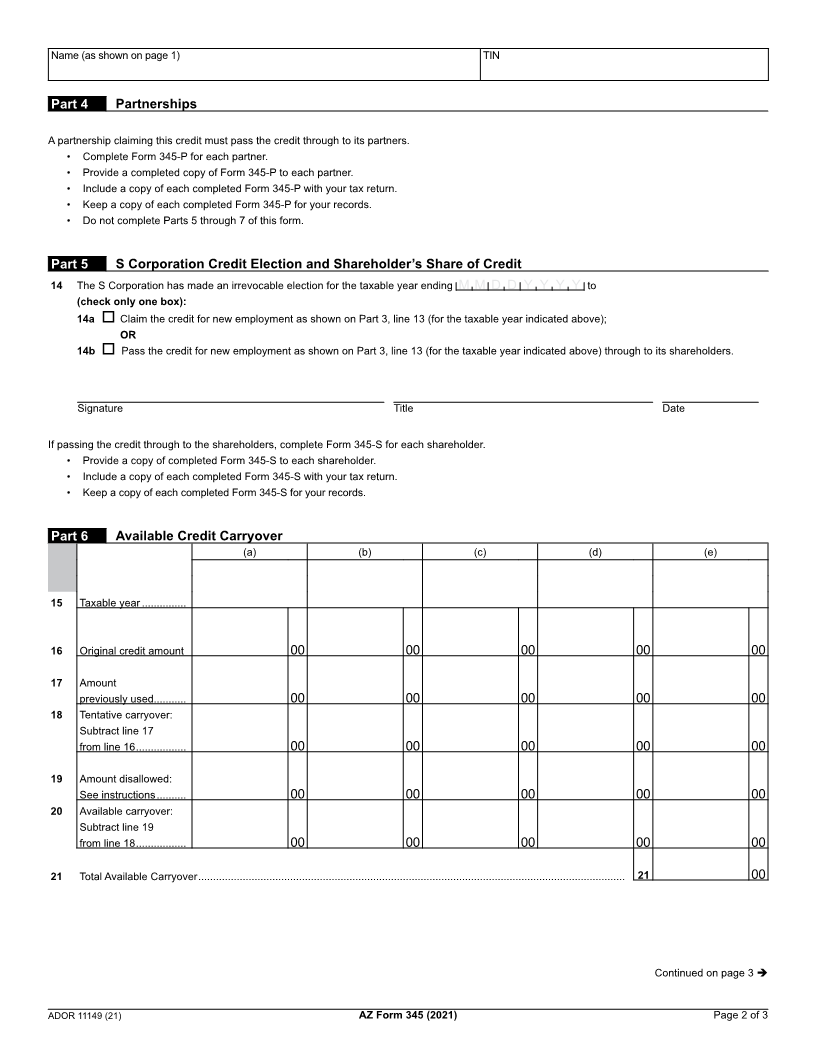
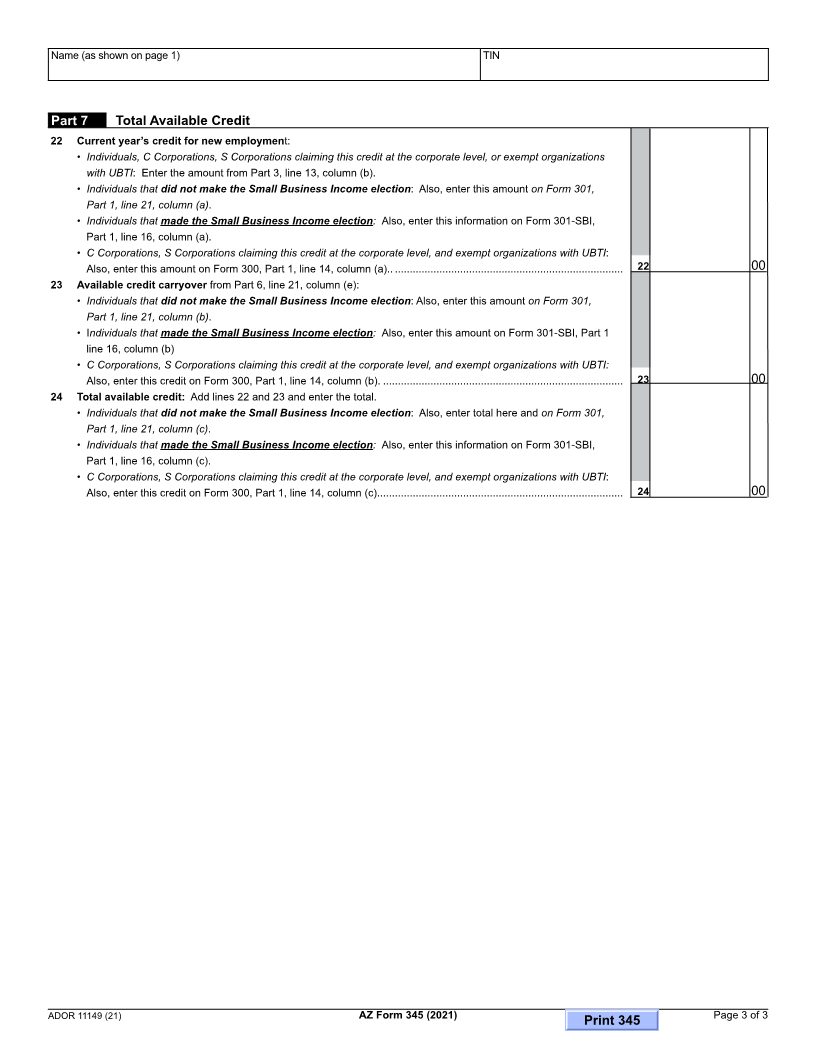
11 Enter the credit passed through from partnerships on Form(s) 345-P, line 3c .................... 11 00
12 Enter the credit passed through from S Corporations on Form(s) 345-S, line 3c................. 12 00
13 Add lines 8 through 12 in column (b). Enter the total. This is your total current year’s
credit for New Employment. ................................................................................................. 13 00
Continued on page 2
ADOR 11149 (21)