Enlarge image
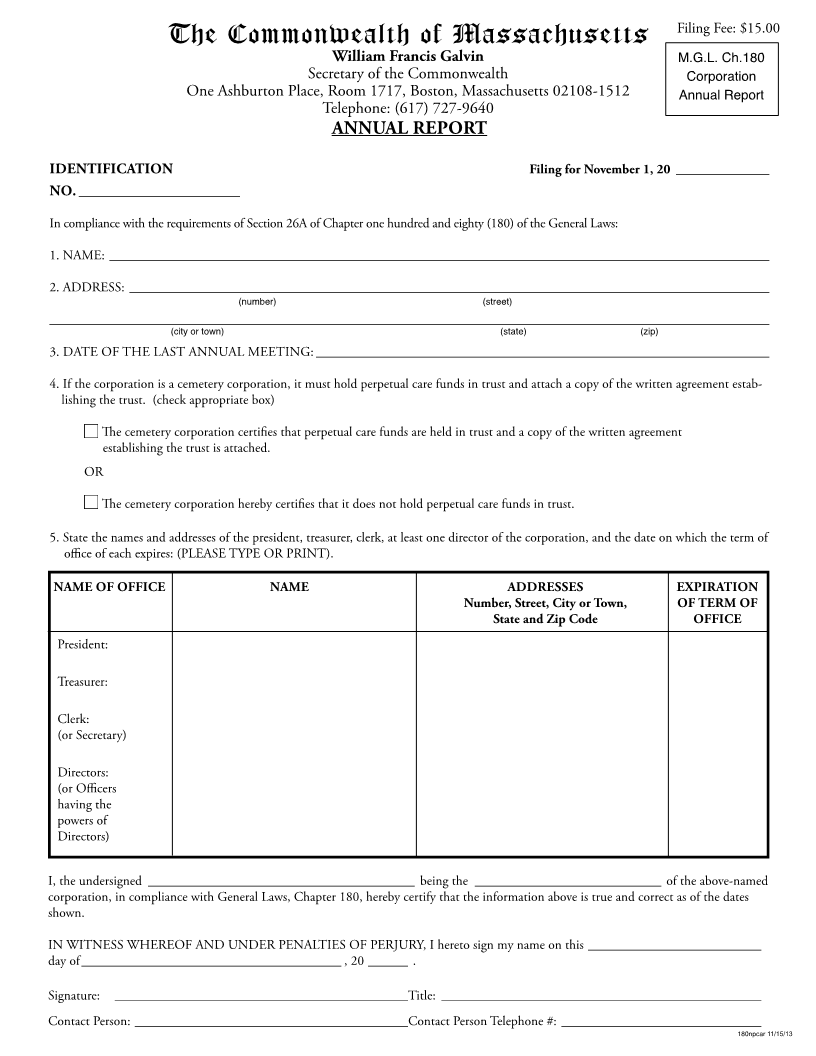
Filing Fee: $15.00
The Commonwealth of Massachusetts
William Francis Galvin M.G.L. Ch.180
Secretary of the Commonwealth Corporation
One Ashburton Place, Room 1717, Boston, Massachusetts 02108-1512 Annual Report
Telephone: (617) 727-9640
ANNUAL REPORT
IDENTIFICATION Filing for November 1, 20 ______________
NO. ______________________
In compliance with the requirements of Section 26A of Chapter one hundred and eighty (180) of the General Laws:
1. NAME: ___________________________________________________________________________________________________
2. ADDRESS: ________________________________________________________________________________________________
(number) (street)
____________________________________________________________________________________________________________
(city or town) (state) (zip)
3. DATE OF THE LAST ANNUAL MEETING: ____________________________________________________________________
4. If the corporation is a cemetery corporation, it must hold perpetual care funds in trust and attach a copy of the written agreement estab-
lishing the trust. (check appropriate box)
The cemetery corporation certifies that perpetual care funds are held in trust and a copy of the written agreement
establishing the trust is attached.
OR
The cemetery corporation hereby certifies that it does not hold perpetual care funds in trust.
5. State the names and addresses of the president, treasurer, clerk, at least one director of the corporation, and the date on which the term of
office of each expires: (PLEASE TYPE OR PRINT).
NAME OF OFFICE NAME ADDRESSES EXPIRATION
Number, Street, City or Town, OF TERM OF
State and Zip Code OFFICE
President:
Treasurer:
Clerk:
(or Secretary)
Directors:
(or Officers
having the
powers of
Directors)
I, the undersigned ________________________________________ being the ____________________________ of the above-named
corporation, in compliance with General Laws, Chapter 180, hereby certify that the information above is true and correct as of the dates
shown.
IN WITNESS WHEREOF AND UNDER PENALTIES OF PERJURY, I hereto sign my name on this __________________________
day of _______________________________________ , 20 ______ .
Signature: ____________________________________________Title: ________________________________________________
Contact Person: _________________________________________Contact Person Telephone #: ______________________________
180npcar 11/15/13