Enlarge image
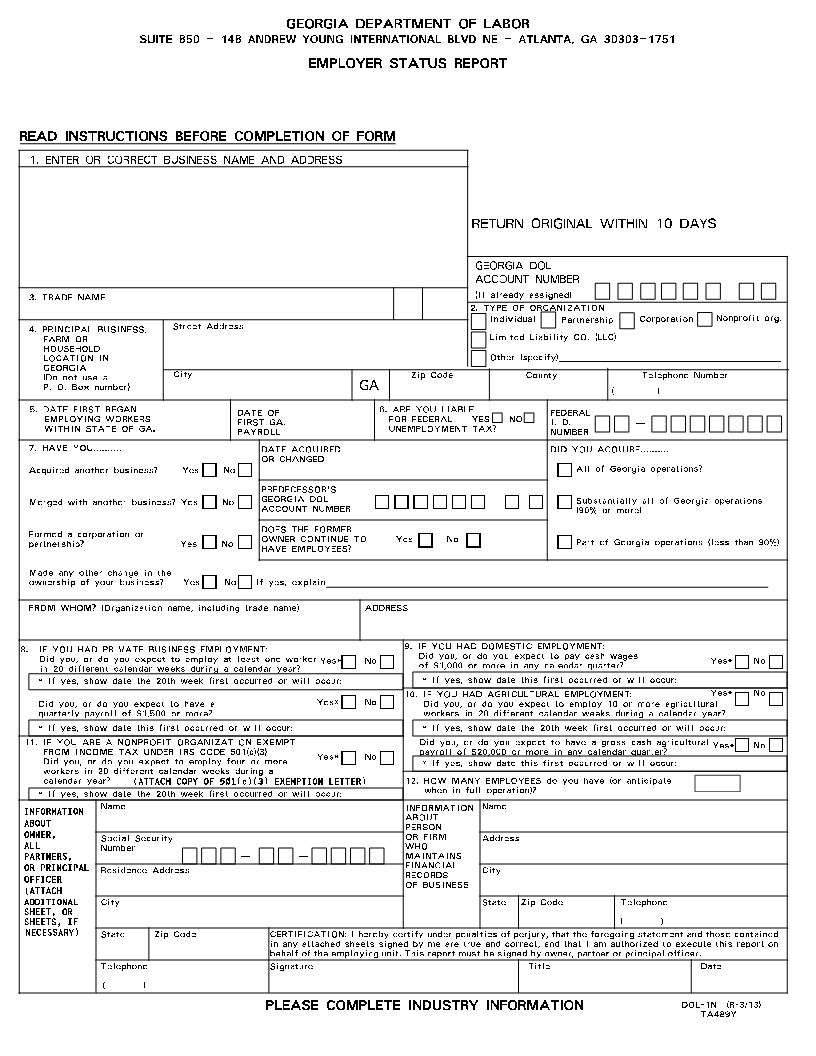
GEORGIA DEPARTMENT OF LABOR
SUITE 850 - 148 ANDREW YOUNG INTERNATIONAL BLVD NE - ATLANTA, GA 30303-1751
EMPLOYER STATUS REPORT
READ INSTRUCTIONS BEFORE COMPLETION OF FORM
1. ENTER OR CORRECT BUSINESS NAME AND ADDRESS
RETURN ORIGINAL WITHIN 10 DAYS
GEORGIA DOL
ACCOUNT NUMBER
_
3. TRADE NAME (If already assigned)
2. TYPE OF ORGANIZATION
4. PRINCIPAL BUSINESS, Street Address Individual Partnership Corporation Nonprofit org.
FARM OR Limited Liability CO. (LLC)
HOUSEHOLD
LOCATION IN Other (specify)________________________
GEORGIA (Do not use a City Zip Code County Telephone Number
P. O. Box number) GA ( )
5. WITHINEMPLOYINGDATE FIRSTSTATEWORKERSBEGANOF GA. DATEFIRSTPAYROLLOFGA. 6.FORUNEMPLOYMENTAREFEDERAL YOU LIABLEYES TAX?NO NUMBERFEDERALI. D. _
7. HAVE YOU.......... DATE ACQUIRED DID YOU ACQUIRE..........
OR CHANGED
Acquired another business? Yes No = = =All of Georgia operations?
PREDECESSOR'S
Merged with another business? Yes No = = ACCOUNTGEORGIA DOLNUMBER ======_ = = =(90%Substantiallyor more)all of Georgia operations
partnership? Formed a corporation or Yes No = = HAVEOWNERDOESEMPLOYEES?THECONTINUEFORMERTO Yes No = = =Part of Georgia operations (less than 90%)
Made any other change in the
ownership of your business? Yes No If yes, explain = =
FROM WHOM? (Organization name, including trade name) ADDRESS
8. DidinIF20YOUyou,differentHADor doPRIVATEcalendaryou expectweeksBUSINESSto employduringEMPLOYMENT:ataleastcalendaroneyear?worker Yes*= No= 9. ofDidIF$1,000YOUyou,HADorordomoreDOMESTICyouinexpectany calendartoEMPLOYMENT:pay cashquarter?wages Yes*=No=
* If yes, show date the 20th week first occurred or will occur: * If yes, show date this first occurred or will occur:
Did you, or do you expect to have a Yes* = No = 10. IF YOU HAD AGRICULTURAL EMPLOYMENT: Did you, or do you expect to employ 10 or more agriculturalYes* = No =
quarterly payroll of $1,500 or more? workers in 20 different calendar weeks during a calendar year?
* If yes, show date this first occurred or will occur: * If yes, show date the 20th week first occurred or will occur:
11. FROMDidIF YOUyou,INCOMEorAREdoAyouNONPROFITTAXexpectUNDERto employIRSORGANIZATIONCODEfour or501(c)(3):moreEXEMPT Yes*= No= * If yes, show dateDidpayrollthisyou,offirstor$20,000dooccurredyouorexpectmoreor willtoinoccur:haveany calendara gross cashquarter?agricultural Yes*=No=
workers in 20 different calendar weeks during a
calendar year? (ATTACH COPY OF 501( )(3) EXEMPTION LETTER)c 12. HOW MANY EMPLOYEES do you have (or anticipate
* If yes, show date the 20th week first occurred or will occur: when in full operation)?
INFORMATIONABOUT Name PERSONABOUTINFORMATION Name
OWNER, Social Security OR FIRM Address
PARTNERS,ALL Number _ _ WHOMAINTAINS
(ATTACHOROFFICERPRINCIPAL Residence Address OFRECORDSFINANCIALBUSINESS City
ADDITIONAL City State Zip Code Telephone
SHEET, OR
SHEETS, IF ( )
NECESSARY) State Zip Code CERTIFICATION: I hereby certify under penalties of perjury, that the foregoing statement and those contained
in any attached sheets signed by me are true and correct, and that I am authorized to execute this report on
behalf of the employing unit. This report must be signed by owner, partner or principal officer.
Telephone Signature Title Date
( )
PLEASE COMPLETE INDUSTRY INFORMATION DOL-1N (R-3/13)
TA489Y