Enlarge image
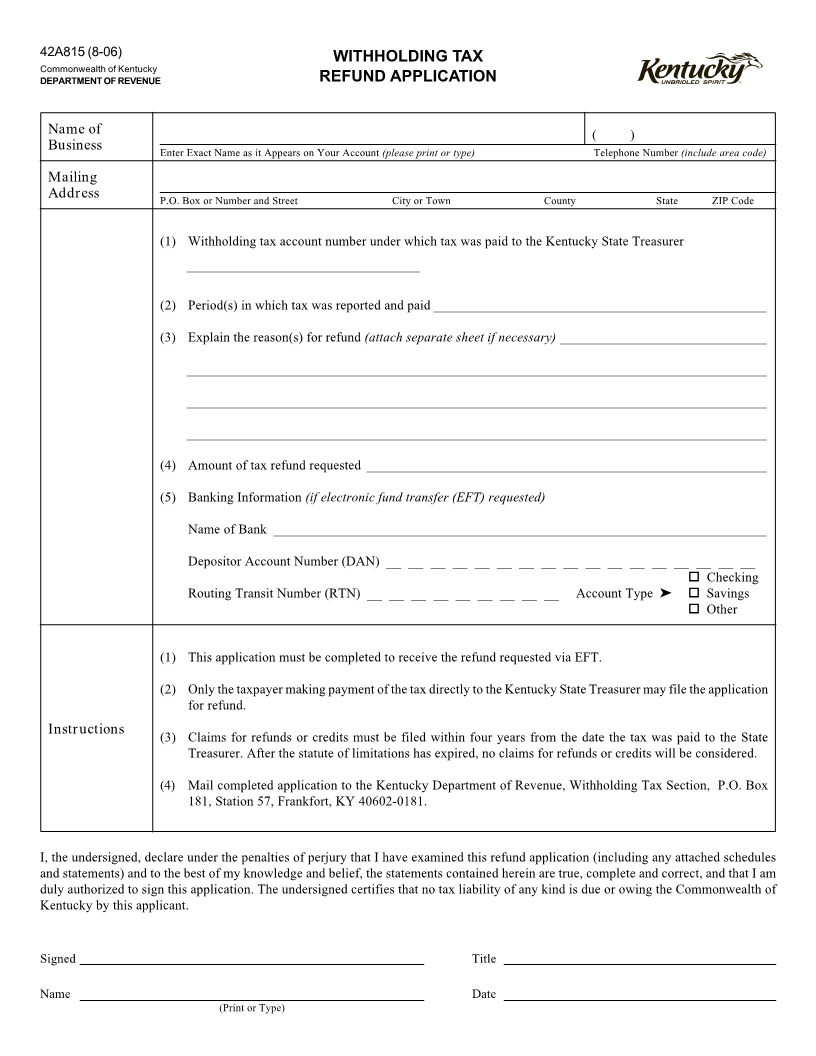
42A815 (8-06) WITHHOLDING TAX
Commonwealth of Kentucky
DEPARTMENT OF REVENUE REFUND APPLICATION
Name of ( )
Business Enter Exact Name as it Appears on Your Account (please print or type) Telephone Number (include area code)
Mailing
Address P.O. Box or Number and Street City or Town County State ZIP Code
(1) Withholding tax account number under which tax was paid to the Kentucky State Treasurer
___________________________________
(2) Period(s) in which tax was reported and paid__________________________________________________
(3) Explain the reason(s) for refund (attach separate sheet if necessary)_______________________________
_______________________________________________________________________________________
_______________________________________________________________________________________
_______________________________________________________________________________________
(4) Amount of tax refund requested ____________________________________________________________
(5) Banking Information (if electronic fund transfer (EFT) requested)
Name of Bank __________________________________________________________________________
Depositor Account Number (DAN) __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __
Checking
Routing Transit Number (RTN) __ __ __ __ __ __ __ __ __ Account Type ➤ Savings
Other
(1) This application must be completed to receive the refund requested via EFT.
(2) Only the taxpayer making payment of the tax directly to the Kentucky State Treasurer may file the application
for refund.
Instructions
(3) Claims for refunds or credits must be filed within four years from the date the tax was paid to the State
Treasurer. After the statute of limitations has expired, no claims for refunds or credits will be considered.
(4) Mail completed application to the Kentucky Department of Revenue, Withholding Tax Section, P.O. Box
181, Station 57, Frankfort, KY 40602-0181.
I, the undersigned, declare under the penalties of perjury that I have examined this refund application (including any attached schedules
and statements) and to the best of my knowledge and belief, the statements contained herein are true, complete and correct, and that I am
duly authorized to sign this application. The undersigned certifies that no tax liability of any kind is due or owing the Commonwealth of
Kentucky by this applicant.
Signed Title
Name Date
(Print or Type)