Enlarge image
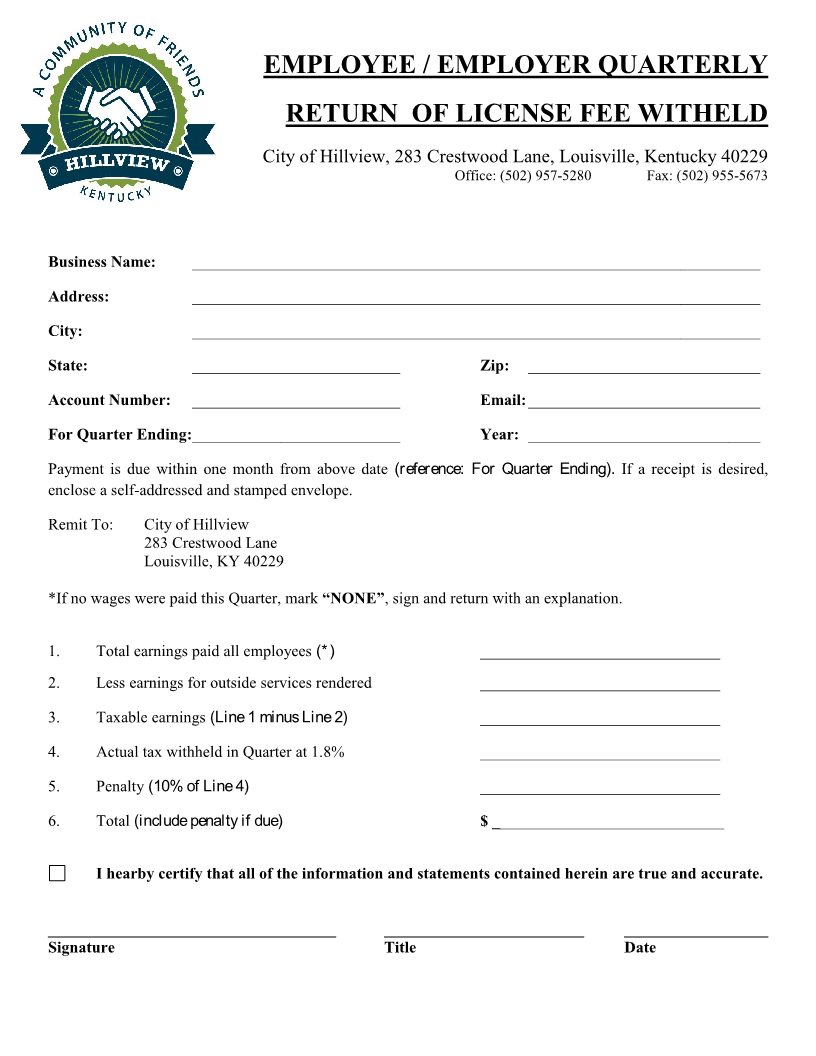
EMPLOYEE / EMPLOYER QUARTERLY
RETURN OF LICENSE FEE WITHELD
City of Hillview, 283 Crestwood Lane, Louisville, Kentucky 40229
Office: (502) 957-5280 Fax: (502) 955-5673
Business Name: _______________________________________________________________________
Address: _______________________________________________________________________
City: _______________________________________________________________________
State: __________________________ Zip: _____________________________
Account Number: __________________________ Email: _____________________________
For Quarter Ending:__________________________ Year: _____________________________
Payment is due within one month from above date (reference: For Quarter Ending). If a receipt is desired,
enclose a self-addressed and stamped envelope.
Remit To: City of Hillview
283 Crestwood Lane
Louisville, KY 40229
*If no wages were paid this Quarter, mark “NONE”, sign and return with an explanation.
1. Total earnings paid all employees (*) ______________________________
2. Less earnings for outside services rendered ______________________________
3. Taxable earnings (Line 1 minus Line 2) ______________________________
4. Actual tax withheld in Quarter at 1.8% ______________________________
5. Penalty (10% of Line 4) ______________________________
6. Total (include penalty if due) $ _____________________________
I hearby certify that all of the information and statements contained herein are true and accurate.
____________________________________ _________________________ __________________
Signature Title Date