Enlarge image
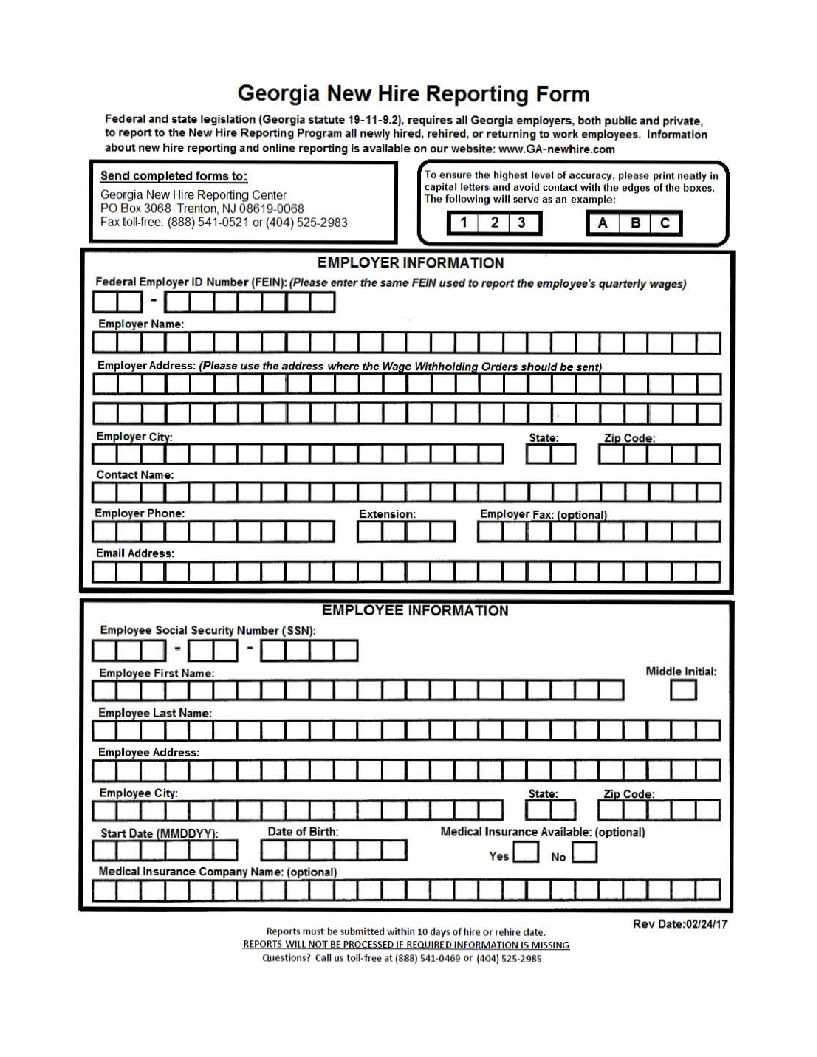
Georgia New Hire Reporting Form
Federaland state legisatl ion (Georgaistatute 19- 1-92)1 . ,requi resallGeorgai employers, both public and priva te,
toreporttothe New H ire ReportingProg r.am allnewylh ired,reh ired ,orreturn ingtoworkempoyeesl . Informatoni
about new hire reporting and onlien reporting is available on ourwebsite:wwwGA. - newhire.com
Send completed forms to: To ensure e th h hig est elve ol f accuracy, plense printneatly In
capi tal lettersandavoidcontact with the edg es of the boxes.
Geo rgai NewHire R·eportingCenter The follow ni g will serve as an exampl e:
PO Box 3068 Tre nton, NJ 08619-0068
Faxtoll-free:(888) 541-0521or (404)525-2983 I1 I2 I3 I ,..-A""'l-B....-C..
EMPLOY ER INFOR M ATION
FederalEmp oyerl ID Number(FEIN):(Pl eauen terthesame FENI usedtoreporttheemployee's quarte yrl wages)
I I 1 1 - I I I I I I I
Employer Name :
EmployerCil State: Zpi Code:
I I I Ir I I I I
Contact Name:
EmployerPhone: Extensio n: Employer Fax :(optional}
I I I I I I I I I I I I
Email Address:
I
EMPLO EEY INFORMATION
Empoyeel Socia l Security Number (SSN):
........____,J ~ I I 1-1 I I
Emf'oyee First Name: Middl eIni itla :
I I I I I D
Employee Last Name :
I I I I I I I
Empoyeel Address:
I I I I I I I ·
Employee City: State: Zip Code:
I I I I I I I I I
Start Date(MMDDVYr Date ofBirth: Medi cal Insurance Available: (opti onal)
I I I I I I I I I ves O ONo
Medcai Insurancel Company Name:(optional)
11111111111
RevDiite:·02/ 24/17
Rep>0rts mustbesubmitted within 10 daysof hrieorreh ire date.
REPORTS WILL NOirBE PRO CESSED IF REQUIRED jNFORMAJ!ON ISM ISSING
Questions? Callus toll-freeat(888} 541·0469 or (404) 525-2985