Enlarge image
COMPLETING PARTS I AND II OF ANNUAL TAX AND WAGE REPORT
FOR DOMESTIC EMPLOYMENT, FORM DOL-4A
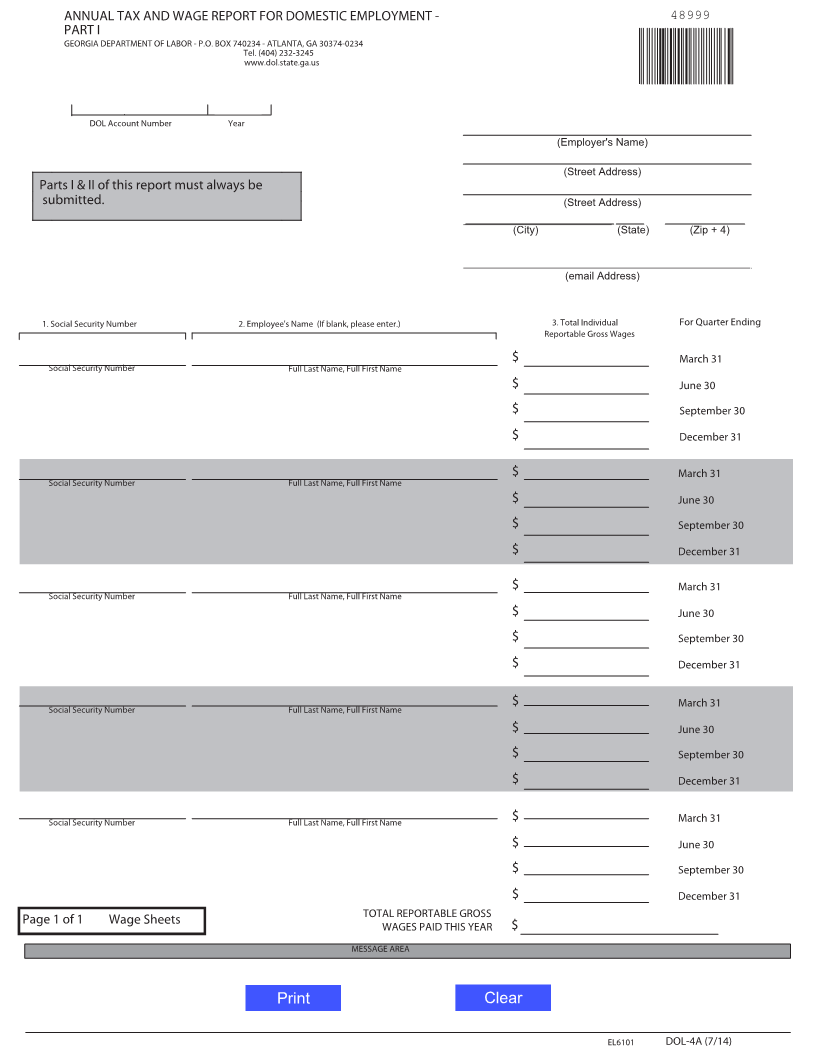
Part I
Enter your DOL account number, the report year, employer name, mailing address, and email
address. Note: If you are a new employer and have not yet been assigned a DOL account
number, enter "Applied For" in the account number field and attach a DOL-1A, Employer
Status Report, if not previously submitted.
Enter the Social Security Number, last name, first name, and total covered wages paid in
each quarter separately. All wages paid to an employee must be reported by the employer
for the quarter in which payment was actually made.
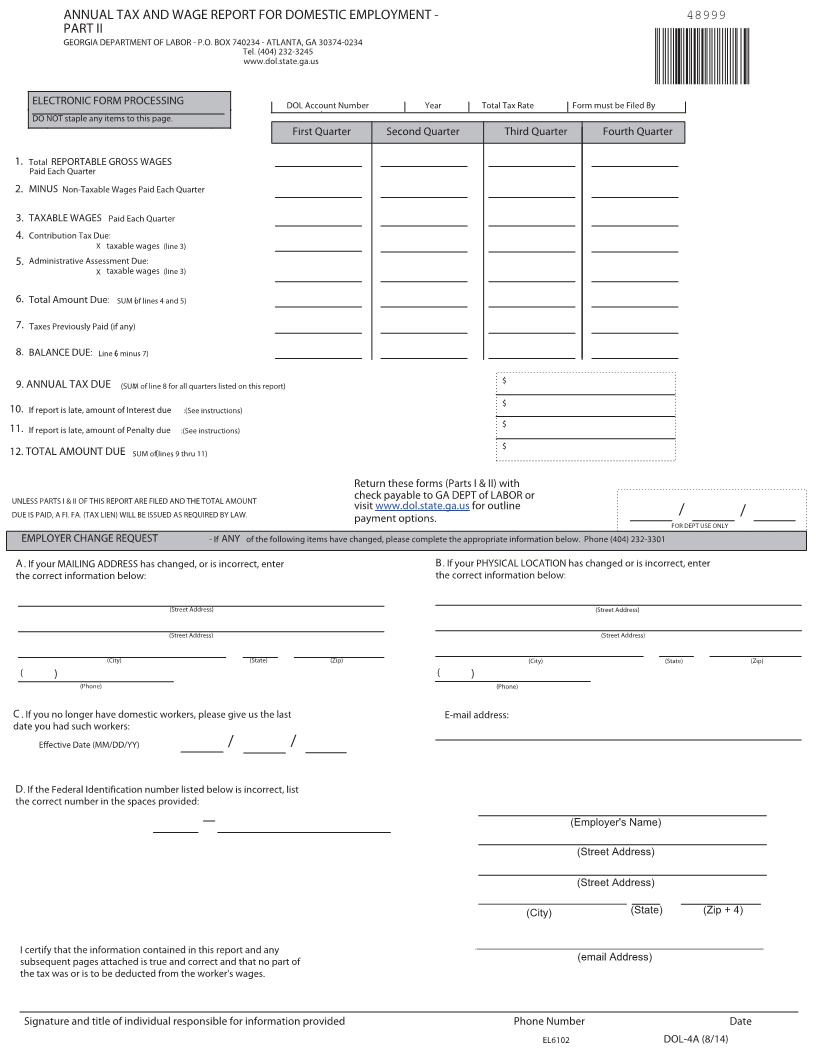
Part II
Line 1 Amount of total reportable gross wages paid for all employees. Show the amount paid
for each quarter separately.
Line 2 Subtract non-taxable wages (amount of wages above $9500 per employee per calendar
year) as applicable for each quarter.
Line 3 Enter the difference between Lines 1 and 2. This amount is used to calculate the
amount of taxes to be paid.
Line 4 In the area provided, enter the Contribution tax rate. To calculate the Contribution tax,
multiply your Contribution tax rate by the amount in Line 3 for each quarter. New
employers must use 2.62%.
Line 5 In the area provided, enter the Administrative Assessment rate. To calculate the
Administrative Assessment tax, multiply the Administrative Assessment rate (.08% or
.0008) by the amount in Line 3 for each quarter. This applies to all employers except
employers with the minimum rate or the maximum rate.
*The total tax rate is contribution + administrative assessment.
Line 6 The sum of Lines 4 and 5 for each quarter.
Line 7 Enter the amount of taxes previously paid for this reporting year.
Line 8 Enter the difference between Lines 6 and 7.
Line 9 The sum of each quarter from Line 8.
Line 10 Interest is computed on the tax due (Line 9) from the due date (January 31) at the rate
of 1.5% per month or fraction of a month. Interest accrues until all tax and
administrative assessments are paid.
Line 11 Enter penalty if the report is filed after January 31. Penalty is $20 or .05% (.0005) of
total wages whichever is greater, for each month the report is late. Compute penalty as
.05% (.0005) of total wages whenever total wages for the quarter are more than
$40,000.
Line 12 Enter the sum of Lines 9 through 11.
Changes in your business information should be reported in Sections A-D at the bottom of Part II.
For assistance with completing Sections A-D, call 404-232-3301. Sign and mail the report,
Parts I and II, no later than January 31.
Visit www.dol.state.ga.us for online payment options or make check or money order payable to
Georgia Department of Labor and provide your DOL account number on your check.
EL6103 DOL-4A Instr. (R-8/14)