Enlarge image
Arizona Form
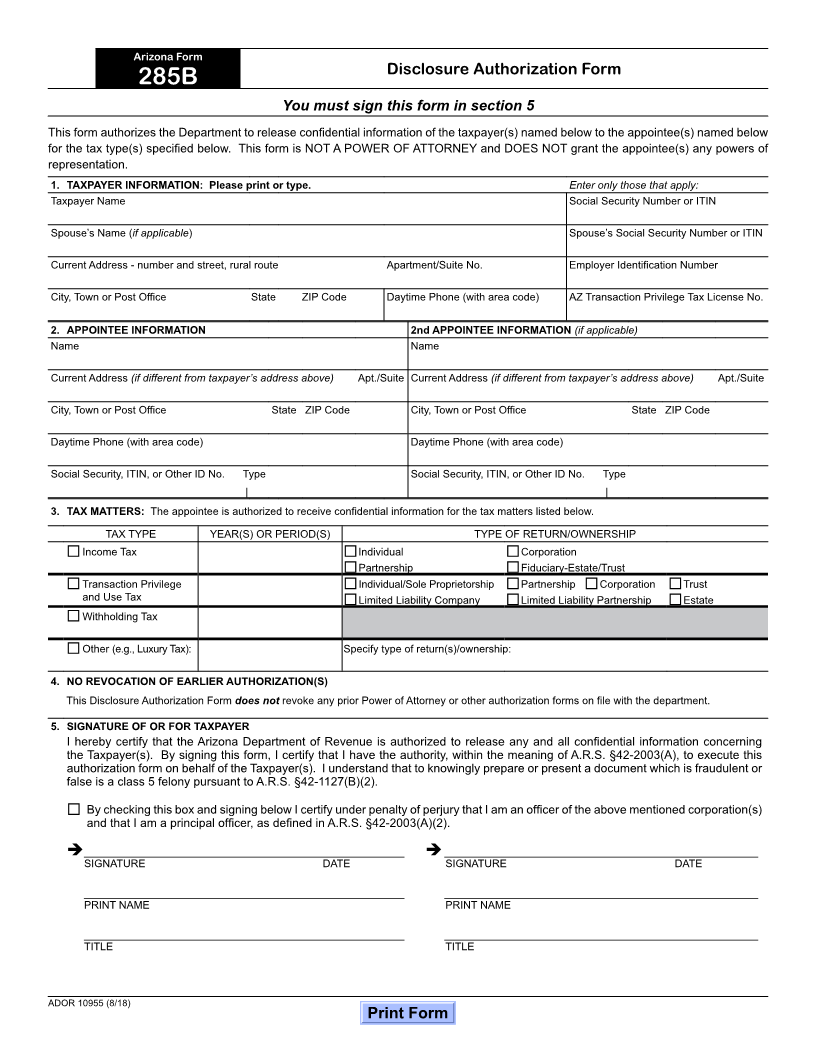
Disclosure Authorization Form
285B
You must sign this form in section 5
This form authorizes the Department to release confidential information of the taxpayer(s) named below to the appointee(s) named below
for the tax type(s) specified below. This form is NOT A POWER OF ATTORNEY and DOES NOT grant the appointee(s) any powers of
representation.
1. TAXPAYER INFORMATION: Please print or type. Enter only those that apply:
Taxpayer Name Social Security Number or ITIN
Spouse’s Name (if applicable) Spouse’s Social Security Number or ITIN
Current Address - number and street, rural route Apartment/Suite No. Employer Identification Number
City, Town or Post Office State ZIP Code Daytime Phone (with area code) AZ Transaction Privilege Tax License No.
2. APPOINTEE INFORMATION 2nd APPOINTEE INFORMATION (if applicable)
Name Name
Current Address (if different from taxpayer’s address above) Apt./Suite Current Address (if different from taxpayer’s address above) Apt./Suite
City, Town or Post Office State ZIP Code City, Town or Post Office State ZIP Code
Daytime Phone (with area code) Daytime Phone (with area code)
Social Security, ITIN, or Other ID No. Type Social Security, ITIN, or Other ID No. Type
| |
3. TAX MATTERS: The appointee is authorized to receive confidential information for the tax matters listed below.
TAX TYPE YEAR(S) OR PERIOD(S) TYPE OF RETURN/OWNERSHIP
Income Tax Individual Corporation
Partnership Fiduciary-Estate/Trust
Transaction Privilege Individual/Sole Proprietorship Partnership Corporation Trust
and Use Tax Limited Liability Company Limited Liability Partnership Estate
Withholding Tax
Other (e.g., Luxury Tax): Specify type of return(s)/ownership:
4. NO REVOCATION OF EARLIER AUTHORIZATION(S)
This Disclosure Authorization Form does not revoke any prior Power of Attorney or other authorization forms on file with the department.
5. SIGNATURE OF OR FOR TAXPAYER
I hereby certify that the Arizona Department of Revenue is authorized to release any and all confidential information concerning
the Taxpayer(s). By signing this form, I certify that I have the authority, within the meaning of A.R.S. §42-2003(A), to execute this
authorization form on behalf of the Taxpayer(s). I understand that to knowingly prepare or present a document which is fraudulent or
false is a class 5 felony pursuant to A.R.S. §42-1127(B)(2).
By checking this box and signing below I certify under penalty of perjury that I am an officer of the above mentioned corporation(s)
and that I am a principal officer, as defined in A.R.S. §42-2003(A)(2).
________________________________________________ _______________________________________________
SIGNATURE DATE SIGNATURE DATE
________________________________________________ _______________________________________________
PRINT NAME PRINT NAME
________________________________________________ _______________________________________________
TITLE TITLE
ADOR 10955 (8/18)
Print Form