Enlarge image
Massachusetts Department of Revenue
Schedule ABIE
Exceptions to the Add Back of Intangible Expenses 2020
Enclose this schedule to claim an exception to the requirement under MGL ch 63, §§ 31I, 31K to add back to net income related member
intangible expenses and costs, including losses incurred in a factoring or discounting transaction. Complete a separate schedule for each
transaction with a related member as to which an exception is claimed.
Name of taxpayer Federal Identification number For tax year beginning Ending
Related member reporting the income Federal Identification number For tax year beginning Ending
Name of jurisdiction(s) in which related member is taxed on net income (if applicable) Unitary business identifier
Principal reporting corporation (if applicable) Federal Identification number For tax year beginning Ending
Deduction claimed is taken on:
Form 355U, Schedule U-E Form 355U, Schedule U-MTI Form 355 or Form 355S, Schedule E Other
Total Exceptions Claimed
11 Amount from Exception 1, line 7. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
12 Amount from Exception 2, line15f. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
13 Amount from Exception 3, line 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
14 Amount from Exception 4, line 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
15 Total add back exception claimed. Add lines 1 through 4. Enter here and on appropriate corporate return. . . . . . . . . . . . 5
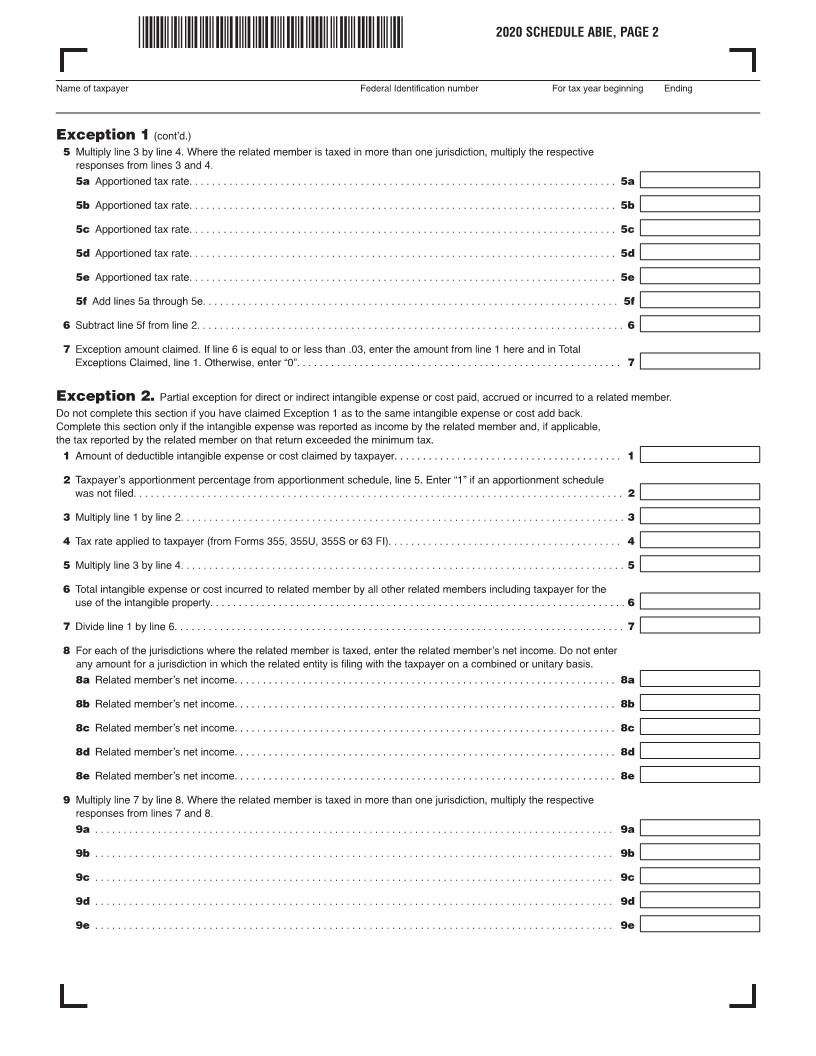
Exception 1
Full exception for direct or indirect intangible expense or cost paid, accrued or incurred to a related member that is
taxed at a similar rate.
11 Amount of deductible intangible expense or cost claimed by taxpayer. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
12 Actual tax rate applied to taxpayer (from Forms 355, 355U, 355S or 63 FI). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
13 Tax rate(s) applied to the corresponding income from intangibles from the related member’s return(s). Do not enter
the tax rate of a jurisdiction in which the related member is filing with the taxpayer on a combined or unitary basis.
1 3a Tax rate from related member’s return. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3a
1 3b Tax rate from related member’s return. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3b
1 3c Tax rate from related member’s return. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3c
1 3d Tax rate from related member’s return. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3d
1 3e Tax rate from related member’s return. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3e
14 Related member apportionment percentage(s) for the jurisdiction(s) referenced in line 3. Enter “1” if the related
member is taxable in only one jurisdiction and therefore not subject to apportionment.
1 4a Related member’s apportionment percentage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4a
1 4b Related member’s apportionment percentage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4b
1 4c Related member’s apportionment percentage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4c
1 4d Related member’s apportionment percentage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4d
1 4e Related member’s apportionment percentage. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4e