Enlarge image
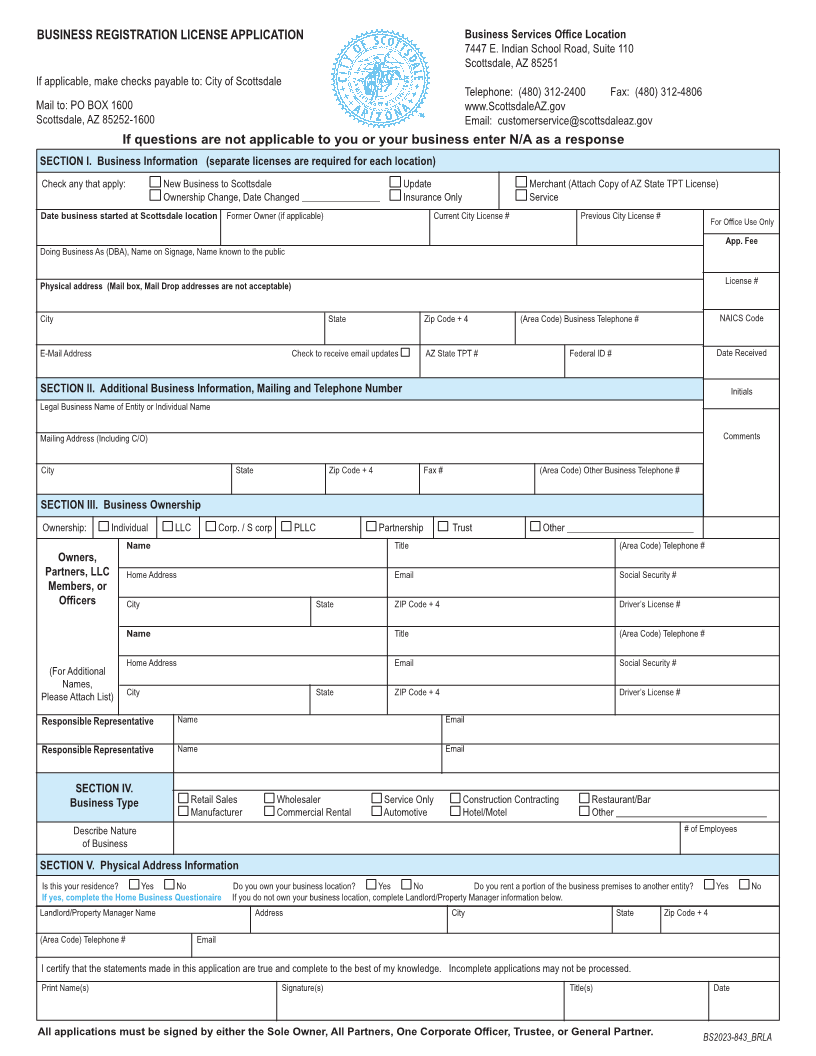
BUSINESS REGISTRATION LICENSE APPLICATION Business Services Office Location
7447 E. Indian School Road, Suite 110
Scottsdale, AZ 85251
If applicable, make checks payable to: City of Scottsdale
Telephone: (480) 312-2400 Fax: (480) 312-4806
Mail to: PO BOX 1600 www.ScottsdaleAZ.gov
Scottsdale, AZ 85252-1600 Email: customerservice@scottsdaleaz.gov
If questions are not applicable to you or your business enter N/A as a response
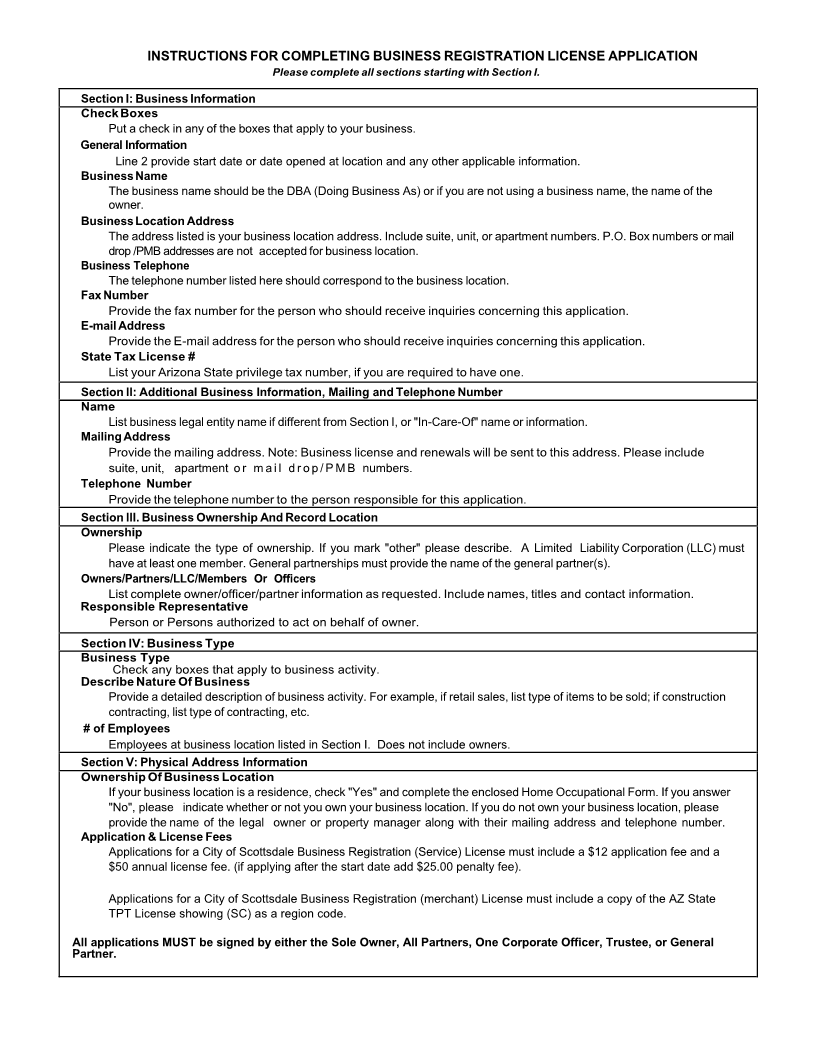
SECTION I. Business Information (separate licenses are required for each location)
Check any that apply: New Business to Scottsdale Update Merchant (Attach Copy of AZ State TPT License)
Ownership Change, Date Changed ________________ Insurance Only Service
Date business started at Scottsdale location Former Owner (if applicable) Current City License # Previous City License # For Office Use Only
App. Fee
Doing Business As (DBA), Name on Signage, Name known to the public
Physical address (Mail box, Mail Drop addresses are not acceptable) License #
City State Zip Code + 4 (Area Code) Business Telephone # NAICS Code
E-Mail Address Check to receive email updates AZ State TPT # Federal ID # Date Received
SECTION II. Additional Business Information, Mailing and Telephone Number Initials
Legal Business Name of Entity or Individual Name
Mailing Address (Including C/O) Comments
City State Zip Code + 4 Fax # (Area Code) Other Business Telephone #
SECTION III. Business Ownership
Ownership: Individual LLC Corp. / S corp PLLC Partnership Trust Other __________________________
Name Title (Area Code) Telephone #
Owners,
Partners, LLC Home Address Email Social Security #
Members, or
Officers City State ZIP Code + 4 Driver’s License #
Name Title (Area Code) Telephone #
Home Address Email Social Security #
(For Additional
Names,
Please Attach List) City State ZIP Code + 4 Driver’s License #
Responsible Representative Name Email
Responsible Representative Name Email
SECTION IV.
Business Type Retail Sales Wholesaler Service Only Construction Contracting Restaurant/Bar
Manufacturer Commercial Rental Automotive Hotel/Motel Other _______________________________
Describe Nature # of Employees
of Business
SECTION V. Physical Address Information
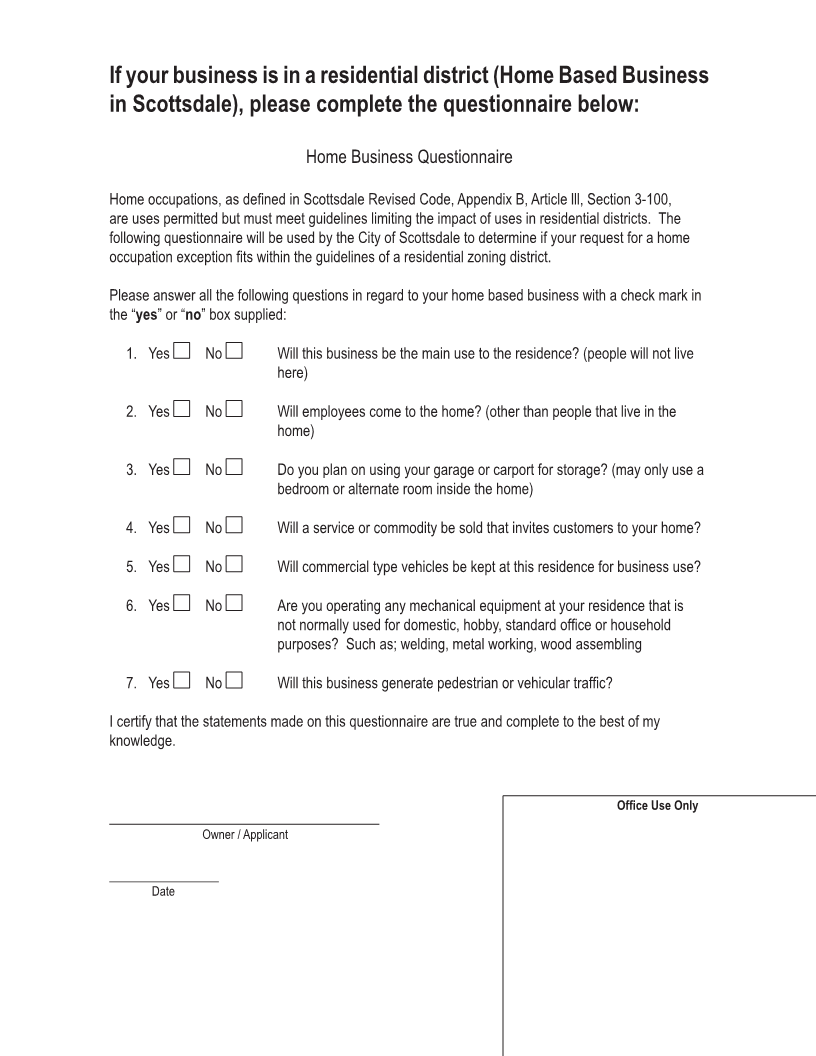
Is this your residence? Yes No Do you own your business location? Yes No Do you rent a portion of the business premises to another entity? Yes No
If yes, complete the Home Business Questionaire If you do not own your business location, complete Landlord/Property Manager information below.
Landlord/Property Manager Name Address City State Zip Code + 4
(Area Code) Telephone # Email
I certify that the statements made in this application are true and complete to the best of my knowledge. Incomplete applications may not be processed.
Print Name(s) Signature(s) Title(s) Date
All applications must be signed by either the Sole Owner, All Partners, One Corporate Officer, Trustee, or General Partner. BS2023-843_BRLA