Enlarge image
UC-514 (03-18) ARIZONA DEPARTMENT OF ECONOMIC SECURITY
Employer Engagement Administration
REPORT OF CHANGES FORM
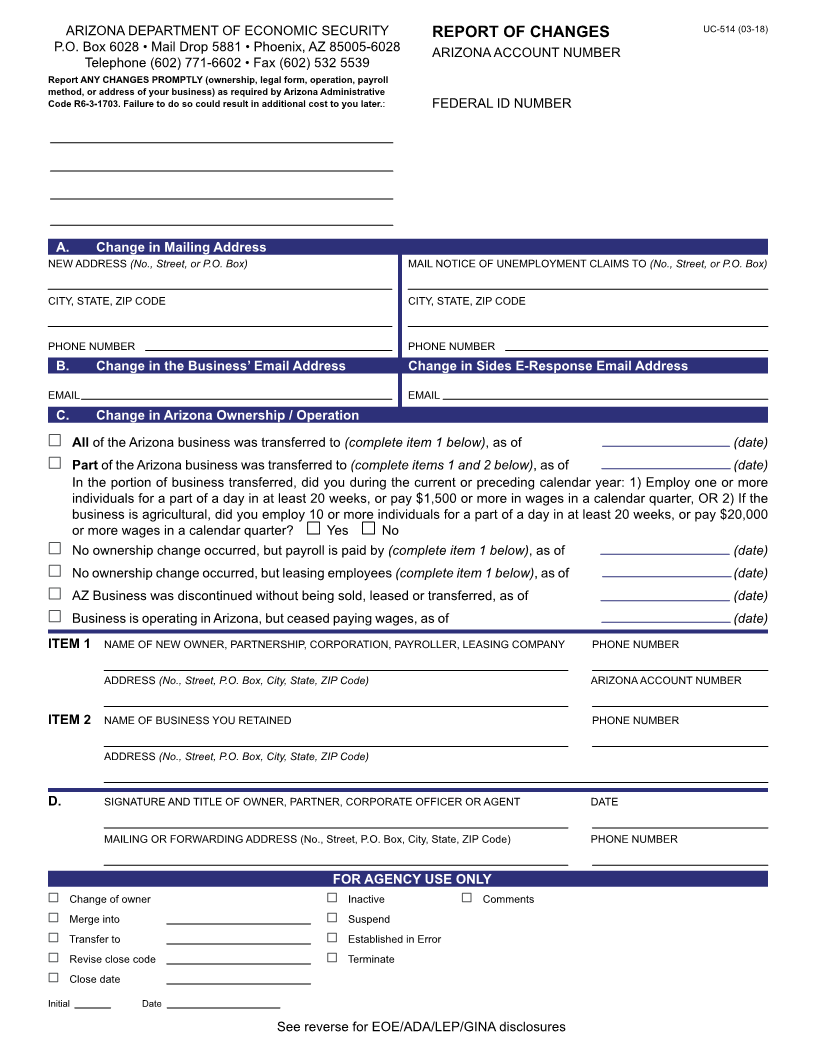
The Report of Changes form is used to advise the Arizona Department of Economic Security of any modifications to
your businessOPERATION or STRUCTURE. You must promptly report any changes inOWNERSHIP,LEGAL FORM ,
OPERATION,PAYROLL METHOD , or ADDRESS of your business. Failure to do so may result in additional costs to
you later.
Your completed form should be mailed or faxed to the address or fax number shown below.
Questions about completing the Report of Changes form or how modifications to your business may affect your UI tax
account should be directed to the Employer Registration Unit at:
Employer Registration Unit
P.O. Box 6028 • Mail Drop 5881
Phoenix, Arizona 85005-6028
Telephone: (602) 771-6602
Fax: (602) 532-5539
Email uitstatus@azdes.gov
Equal Opportunity Employer/Program • Under Titles VI and VII of the Civil Rights Act of 1964 (Title VI & VII), and the
Americans with Disabilities Act of 1990 (ADA), Section 504 of the Rehabilitation Act of 1973, the Age Discrimination
Act of 1975, and Title II of the Genetic Information Nondiscrimination Act (GINA) of 2008; the Department prohibits
discrimination in admissions, programs, services, activities, or employment based on race, color, religion, sex, national
origin, age, disability, genetics and retaliation. The Department must make a reasonable accommodation to allow a
person with a disability to take part in a program, service, or activity. Auxiliary aids and services are available upon
request to individuals with disabilities. To request this document in alternative format or for further information about
this policy, Contact the UI Tax Office at 602-771-6606; TTY/TDD Services: 7-1-1. • Free language assistance for DES
services is available upon request.