Enlarge image
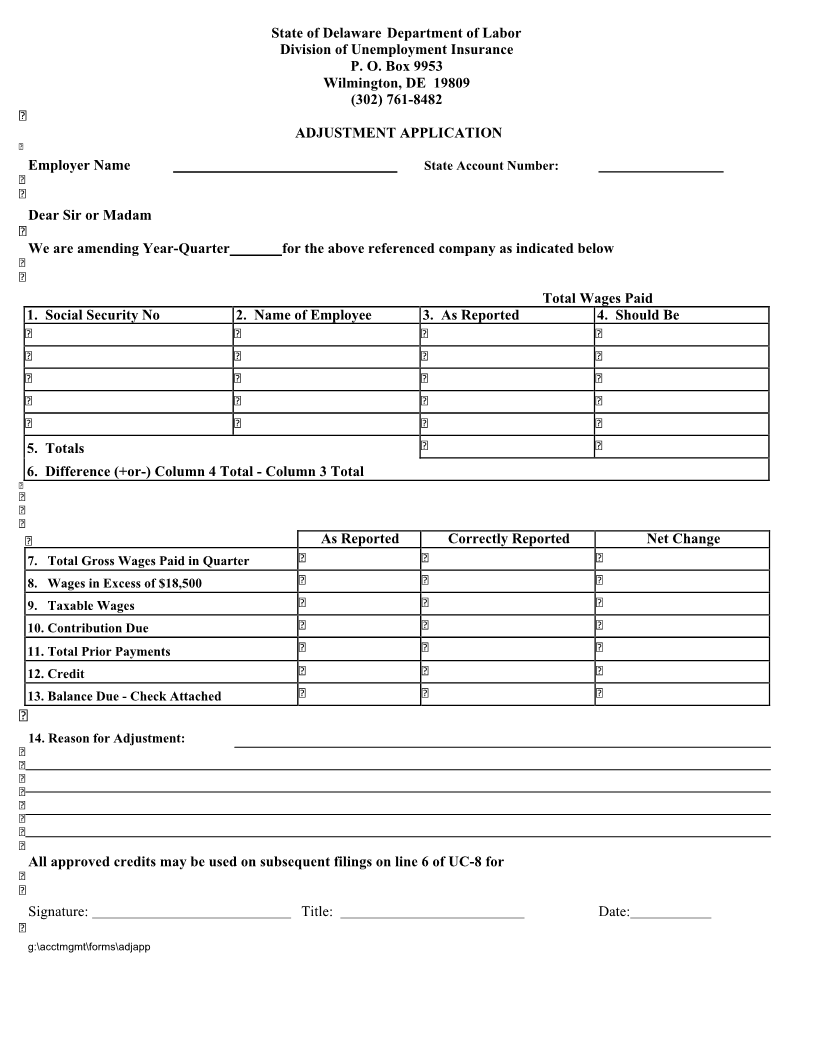
State of Delaware Department of Labor
Division of Unemployment Insurance
P. O. Box 9953
Wilmington, DE 19809
(302) 761-8482
ADJUSTMENT APPLICATION
Employer Name State Account Number:
Dear Sir or Madam
We are amending Year-Quarter for the above referenced company as indicated below
Total Wages Paid
1. Social Security No 2. Name of Employee 3. As Reported 4. Should Be
5. Totals
6. Difference (+or-) Column 4 Total - Column 3 Total
As Reported Correctly Reported Net Change
7. Total Gross Wages Paid in Quarter
8. Wages in Excess of $18,500
9. Taxable Wages
10. Contribution Due
11. Total Prior Payments
12. Credit
13. Balance Due - Check Attached
14. Reason for Adjustment:
All approved credits may be used on subsequent filings on line 6 of UC-8 for
Signature: Title: Date:
g:\acctmgmt\forms\adjapp