Enlarge image
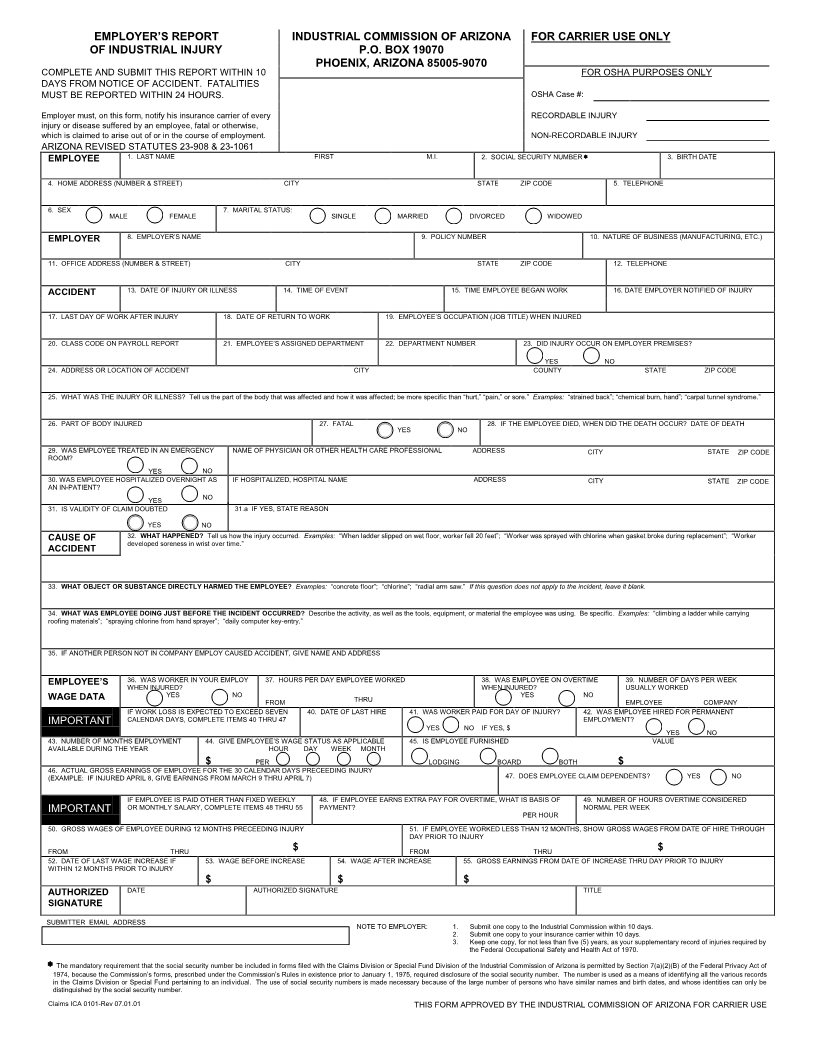
EMPLOYER’S REPORT INDUSTRIAL COMMISSION OF ARIZONA FOR CARRIER USE ONLY
OF INDUSTRIAL INJURY P.O. BOX 19070
PHOENIX, ARIZONA 85005-9070
COMPLETE AND SUBMIT THIS REPORT WITHIN 10 FOR OSHA PURPOSES ONLY
DAYS FROM NOTICE OF ACCIDENT. FATALITIES
MUST BE REPORTED WITHIN 24 HOURS. OSHA Case #:
Employer must, on this form, notify his insurance carrier of every RECORDABLE INJURY
injury or disease suffered by an employee, fatal or otherwise,
which is claimed to arise out of or in the course of employment. NON-RECORDABLE INJURY
ARIZONA REVISED STATUTES 23-908 & 23-1061
EMPLOYEE 1. LAST NAME FIRST M.I. 2. SOCIAL SECURITY NUMBER 3. BIRTH DATE
4. HOME ADDRESS (NUMBER & STREET) CITY STATE ZIP CODE 5. TELEPHONE
6. SEX MALE FEMALE 7. MARITAL STATUS: SINGLE MARRIED DIVORCED WIDOWED
EMPLOYER 8. EMPLOYER’S NAME 9. POLICY NUMBER 10. NATURE OF BUSINESS (MANUFACTURING, ETC.)
11. OFFICE ADDRESS (NUMBER & STREET) CITY STATE ZIP CODE 12. TELEPHONE
ACCIDENT 13. DATE OF INJURY OR ILLNESS 14. TIME OF EVENT 15. TIME EMPLOYEE BEGAN WOR K 16.DATE EMPLOYER NOTIFIED OF INJURY
17. LAST DAY OF WORK AFTER INJURY 18. DATE OF RETURN TO WORK 19. EMPLOYEE’S OCCUPATION (JOB TITLE) WHEN INJURED
20. CLASS CODE ON PAYROLL REPORT 21. EMPLOYEE’S ASSIGNED DEPARTMENT 22. DEPARTMENT NUMBER 23. DID INJURY OCCUR ON EMPLOYER PREMISES?
YES NO
24. ADDRESS OR LOCATION OF ACCIDENT CITY COUNTY STATE ZIP CODE
25. WHAT WAS THE INJURY OR ILLNESS? Tell us the part of the body that was affected and how it was affected; be more specific than “hurt,” “pain,” or sore.” Examples: “strained back”; “chemical burn, hand”; “carpal tunnel syndrome.”
26. PART OF BODY INJURED 27. FATAL YES NO 28. IF THE EMPLOYEE DIED, WHEN DID THE DEATH OCCUR? DATE OF DEATH
29. WAS EMPLOYEE TREATED IN AN EMERGENCY NAME OF PHYSICIAN OR OTHER HEALTH CARE PROFESSIONAL ADDRESS CITY STATE ZIP CODE
ROOM?
YES NO
30.WAS EMPLOYEE HOSPITALIZED OVERNIGHT AS IF HOSPITALIZED, HOSPITAL NAME ADDRESS CITY STATE ZIP CODE
AN IN-PATIENT?
YES NO
31. IS VALIDITY OF CLAIM DOUBTED 31.a IF YES,STATE REASON
YES NO
CAUSE OF 32. WHAT HAPPENED? Tell us how the injury occurred. Examples: “When ladder slipped on wet floor, worker fell 20 feet”; “Worker was sprayed with chlorine when gasket broke during replacement”; “Worker
ACCIDENT developed soreness in wrist over time.”
33. WHAT OBJECT OR SUBSTANCE DIRECTLY HARMED THE EMPLOYEE? Examples: “concrete floor”; “chlorine”; “radial arm saw.” If this question does not apply to the incident, leave it blank.
34. WHAT WAS EMPLOYEE DOING JUST BEFORE THE INCIDENT OCCURRED? Describe the activity, as well as the tools, equipment, or material the employee was using. Be specific. Examples: “climbing a ladder while carrying
roofing materials”; “spraying chlorine from hand sprayer”; “daily computer key-entry.”
35. IF ANOTHER PERSON NOT IN COMPANY EMPLOY CAUSED ACCIDENT, GIVE NAME AND ADDRESS
EMPLOYEE’S 36. WAS WORKER IN YOUR EMPLOY 37. HOURS PER DAY EMPLOYEE WORKED 38. WAS EMPLOYEE ON OVERTIME 39. NUMBER OF DAYS PER WEEK
WHEN INJURED? WHEN INJURED? USUALLY WORKED
WAGE DATA YES NO THRU YES NO EMPLOYEEJURY
FROM EMPLOYEE COMPANY
IF WORK LOSS IS EXPECTED TO EXCEED SEVEN 40. DATE OF LAST HIRE 41. WAS WORKER PAID FOR DAY OF INJURY? 42. WAS EMPLOYEE HIRED FOR PERMANENT
IMPORTANT CALENDAR DAYS, COMPLETE ITEMS 40 THRU 47 EMPLOYMENT?
YES NO IF YES, $ YES NO
43. NUMBER OF MONTHS EMPLOYMENT 44. GIVE EMPLOYEE’S WAGE STATUS AS APPLICABLE 45. IS EMPLOYEE FURNISHED VALUE
AVAILABLE DURING THE YEAR HOUR DAY WEEK MONTH
$ PER LODGING BOARD BOTH $
46. ACTUAL GROSS EARNINGS OF EMPLOYEE FOR THE 30 CALENDAR DAYS PRECEEDING INJURY 47. DOES EMPLOYEE CLAIM DEPENDENTS? YES NO
(EXAMPLE: IF INJURED APRIL 8, GIVE EARNINGS FROM MARCH 9 THRU APRIL 7)
IF EMPLOYEE IS PAID OTHER THAN FIXED WEEKLY 48. IF EMPLOYEE EARNS EXTRA PAY FOR OVERTIME, WHAT IS BASIS OF 49. NUMBER OF HOURS OVERTIME CONSIDERED
IMPORTANT OR MONTHLY SALARY, COMPLETE ITEMS 48 THRU 55 PAYMENT? NORMAL PER WEEK
PER HOUR
50. GROSS WAGES OF EMPLOYEE DURING 12 MONTHS PRECEEDING INJURY 51. IF EMPLOYEE WORKED LESS THAN 12 MONTHS, SHOW GROSS WAGES FROM DATE OF HIRE THROUGH
DAY PRIOR TO INJURY
FROM THRU $ FROM THRU $
52. DATE OF LAST WAGE INCREASE IF 53. WAGE BEFORE INCREASE 54. WAGE AFTER INCREASE 55. GROSS EARNINGS FROM DATE OF INCREASE THRU DAY PRIOR TO INJURY
WITHIN 12 MONTHS PRIOR TO INJURY
$ $ $
AUTHORIZED DATE AUTHORIZED SIGNATURE TITLE
SIGNATURE
SUBMITTER EMAIL ADDRESS NOTE TO EMPLOYER: 1. Submit one copy to the Industrial Commission within 10 days.
2. Submit one copy to your insurance carrier within 10 days.
3. Keep one copy, for not less than five (5) years, as your supplementary record of injuries required by
the Federal Occupational Safety and Health Act of 1970.
The mandatory requirement that the social security number be included in forms filed with the Claims Division or Special Fund Division of the Industrial Commission of Arizona is permitted by Section 7(a)(2)(B) of the Federal Privacy Act of
1974, because the Commission’s forms, prescribed under the Commission’s Rules in existence prior to January 1, 1975, required disclosure of the social security number. The number is used as a means of identifying all the various records
in the Claims Division or Special Fund pertaining to an individual. The use of social security numbers is made necessary because of the large number of persons who have similar names and birth dates, and whose identities can only be
distinguished by the social security number.
Claims ICA 0101-Rev 07.01.01 THIS FORM APPROVED BY THE INDUSTRIAL COMMISSION OF ARIZONA FOR CARRIER USE