Enlarge image
UIT-1146A FORFF (4-18) ARIZONA DEPARTMENT OF ECONOMIC SECURITY
Employer Engagement Administration
LIMITED POWER OF ATTORNEY
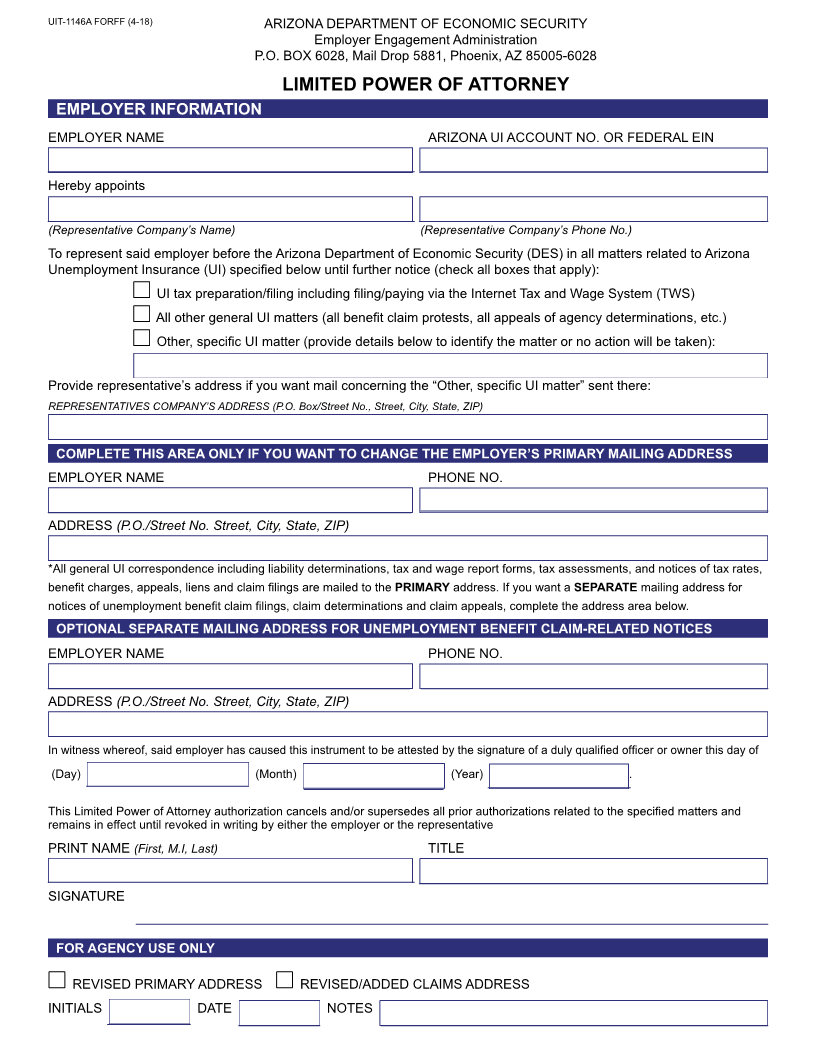
The Limited Power of Attorney form is used by employers to authorize a third party to represent them before the Arizona
Department of Economic Security (DES) in the Unemployment Insurance (UI) matters specified on the form. Such
authorization also permits DES to provide the representative with any confidential information concerning the employer’s
Arizona UI account that is related to those matters.
Specify which matters the authorization applies to by checking the appropriate checkbox(es) on the form. If you want
the authorization limited to a specific matter, such as a specific DES decision under appeal, check the “Other, specific UI
matter” checkbox and briefly describe the matter in the space below to identify it specifically. Provide the representative’s
address immediately below that if you want to have all correspondence related to the “Other, specific UI matter” mailed to
that address.
If you want to change the primary mailing address for general DES correspondence related to the employer’s UI account,
complete the area of the form provided for that purpose. You may also specify a separate mailing address for unemployment
benefit claim-related notices by completing the area of the form provided for that purpose. Such a separate address is
sometimes advisable, to enable the timely protesting of claims. Protests must be returned or postmarked within 10 business
days after the date on the claim filing notice (Notice to Employer – UB-110) to be considered timely.
Submit the completed form with the original signature of a duly qualified officer or owner of the employer’s business to the
UI Tax Employer Registration Unit at the address below. Questions about the use or completion of the form should also be
directed to the Employer Registration Unit.
ADES - UI Tax Section
Employer Registration Unit
P.O. Box 6028 - Mail Drop 5881
Phoenix, Arizona 85005-6028
Telephone – (602) 771-6602
Fax – (602) 532-5539
Email – UITStatusClerical@azdes.gov
Equal Opportunity Employer/Program • Under Titles VI and VII of the Civil Rights Act of 1964 (Title VI & VII), and the
Americans with Disabilities Act of 1990 (ADA), Section 504 of the Rehabilitation Act of 1973, the Age Discrimination Act of
1975, and Title II of the Genetic Information Nondiscrimination Act (GINA) of 2008; the Department prohibits discrimination in
admissions, programs, services, activities, or employment based on race, color, religion, sex, national origin, age, disability,
genetics and retaliation. The Department must make a reasonable accommodation to allow a person with a disability to take
part in a program, service, or activity. Auxiliary aids and services are available upon request to individuals with disabilities.
To request this document in alternative format or for further information about this policy, Contact the UI Tax Office at 602-
771-6606; TTY/TDD Services: 7-1-1. • Free language assistance for DES services is available upon request. • Disponible
en español en línea o en la oficina local.