Enlarge image
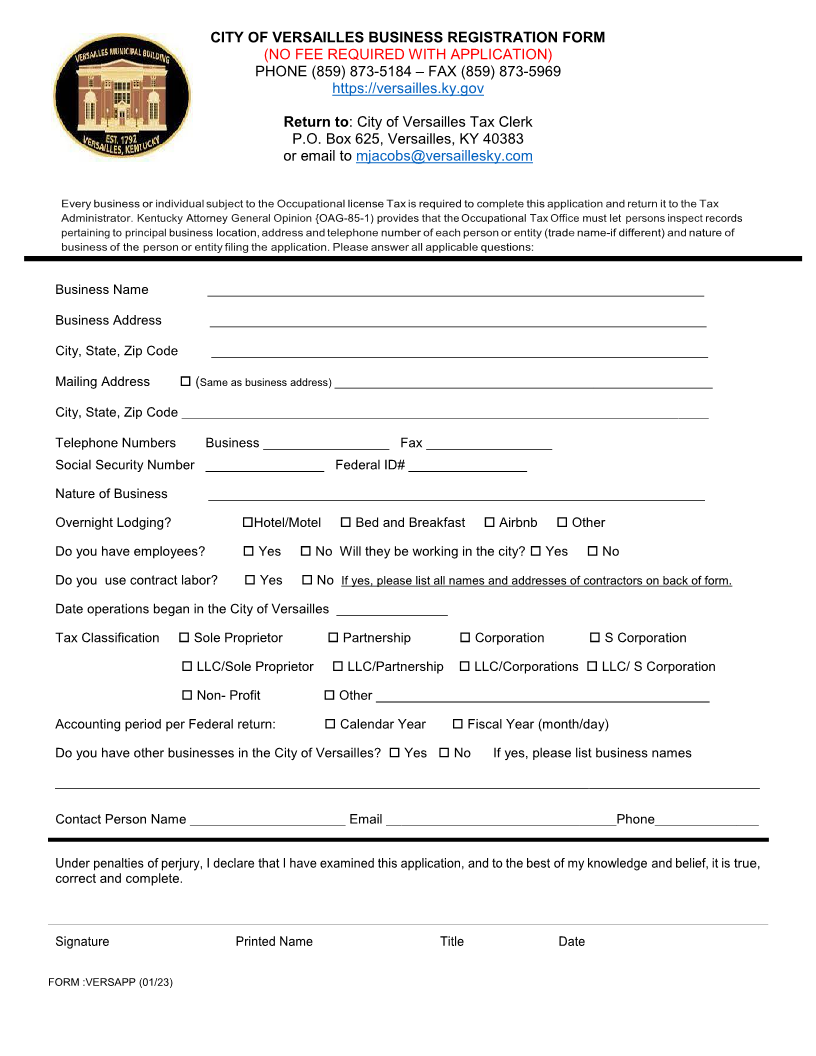
CITY OF VERSAILLES BUSINESS REGISTRATION FORM
(NO FEE REQUIRED WITH APPLICATION)
PHONE (859) 873-5184 – FAX (859) 873-5969
https://versailles.ky.gov
Return to: City of Versailles Tax Clerk
P.O. Box 625, Versailles, KY 40383
or email to mjacobs@versaillesky.com
Every business or individual subject to the Occupational license Tax requiredis to completethisapplication and return toitthe Tax
Administrator. Kentucky Attorney General Opinion {OAG-85-1) provides that the Occupational Tax Office must let persons inspect records
pertainingto principalbusiness location,address and telephone numberof each person or entity (tradename-if different) andnatureof
business of the person or entity filing the application. Please answer all applicable questions:
Business Name ___________________________________________________________________
Business Address ___________________________________________________________________
City, State, Zip Code ___________________________________________________________________
Mailing Address ( Same as business address)___________________________________________________
City, State, Zip Code _______________________________________________________________________
Telephone Numbers Business _________________ Fax _________________
Social Security Number ________________ Federal ID# ________________
Nature of Business ___________________________________________________________________
Overnight Lodging? Hotel/Motel Bed and Breakfast Airbnb Other
Do you have employees? Yes No Will they be working in the city? Yes No
Do you use contract labor? Yes No If yes, please list all names and addresses of contractors on back of form.
Date operations began in the City of Versailles _______________
Tax Classification Sole Proprietor Partnership Corporation S Corporation
LLC/Sole Proprietor LLC/Partnership LLC/Corporations LLC/ S Corporation
Non- Profit Other_____________________________________________
Accounting period per Federal return: Calendar Year Fiscal Year (month/day)
Do you have other businesses in the City of Versailles? Yes No If yes, please list business names
_______________________________________________________________________________________________
Contact Person Name _____________________ Email _______________________________Phone______________
Under penalties of perjury, I declare that I have examined this application, and to the best of my knowledge and belief,true,it is
correct and complete.
Signature Printed Name Title Date
FORM :VERSAPP (01/23)