Enlarge image
Fax: (859) 387-7651
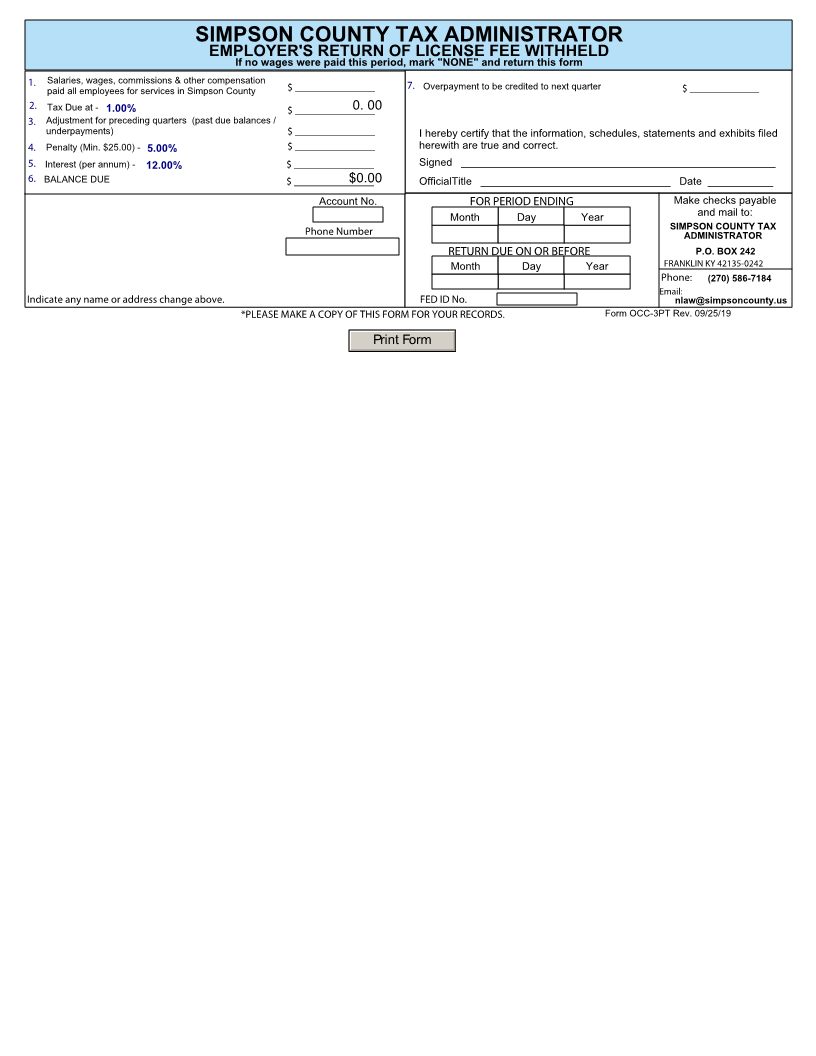
SIMPSON COUNTY TAX ADMINISTRATOR
EMPLOYER'S RETURN OF LICENSE FEE WITHHELD
If no wages were paid this period, mark "NONE" and return this form
1. Salaries, wages, commissions & other compensation 7. Overpayment to be credited to next quarter $ _____________
paid all employees for services in Simpson County $ _______________
2. Tax Due at - 1.00% $ _______________0. 00
3. Adjustment for preceding quarters (past due balances /
underpayments) $ _______________ I hereby certify that the information, schedules, statements and exhibits filed
4. Penalty (Min. $25.00) - 5.00% $ _______________ herewith are true and correct.
5. Interest (per annum) - 12.00% $ _______________ Signed _____________________________________________________
6. BALANCE DUE $ _______________ $0.00 OfficialTitle ________________________________ Date ___________
Account No. FOR PERIOD ENDING Make checks payable
Month Day Year and mail to:
Phone Number SIMPSON COUNTY TAX
ADMINISTRATOR
RETURN DUE ON OR BEFORE P.O. BOX 242
Month Day Year FRANKLIN KY 42135-0242
Phone: (270) 586-7184
Email:
Indicate any name or address change above. FED ID No. nlaw@simpsoncounty.us
*PLEASE MAKE A COPY OF THIS FORM FOR YOUR RECORDS. Form OCC-3PT Rev. 09/25/19
Print Form