Enlarge image
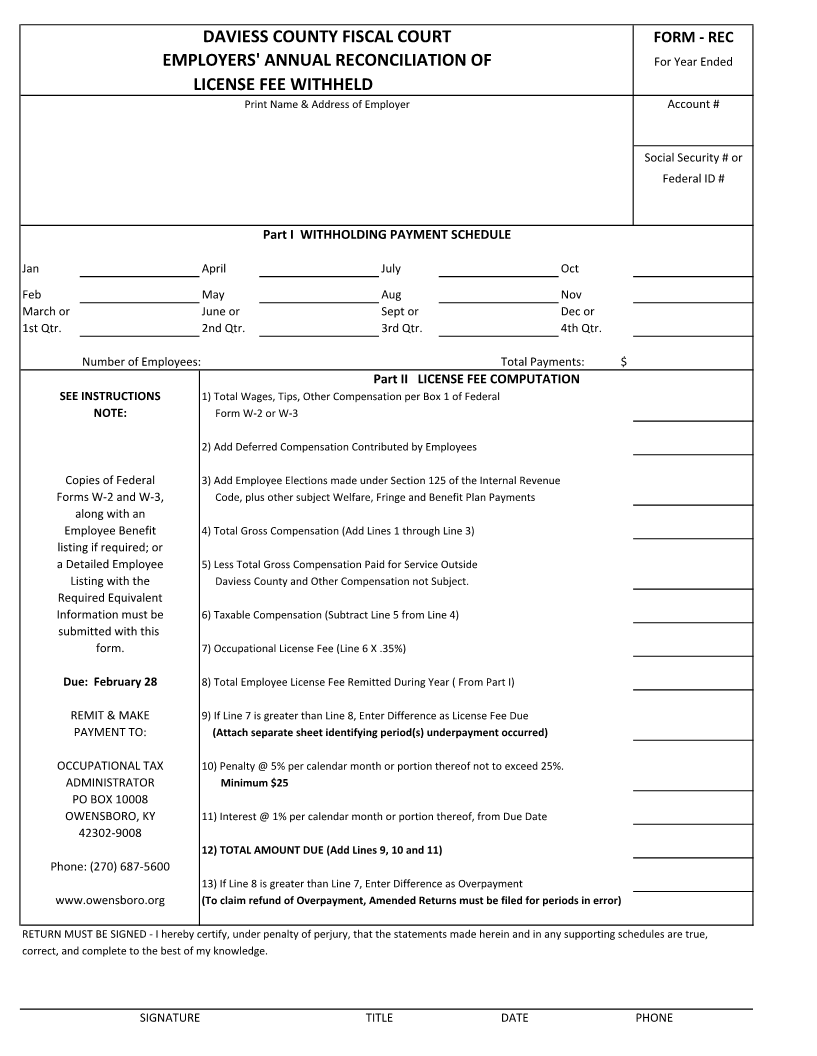
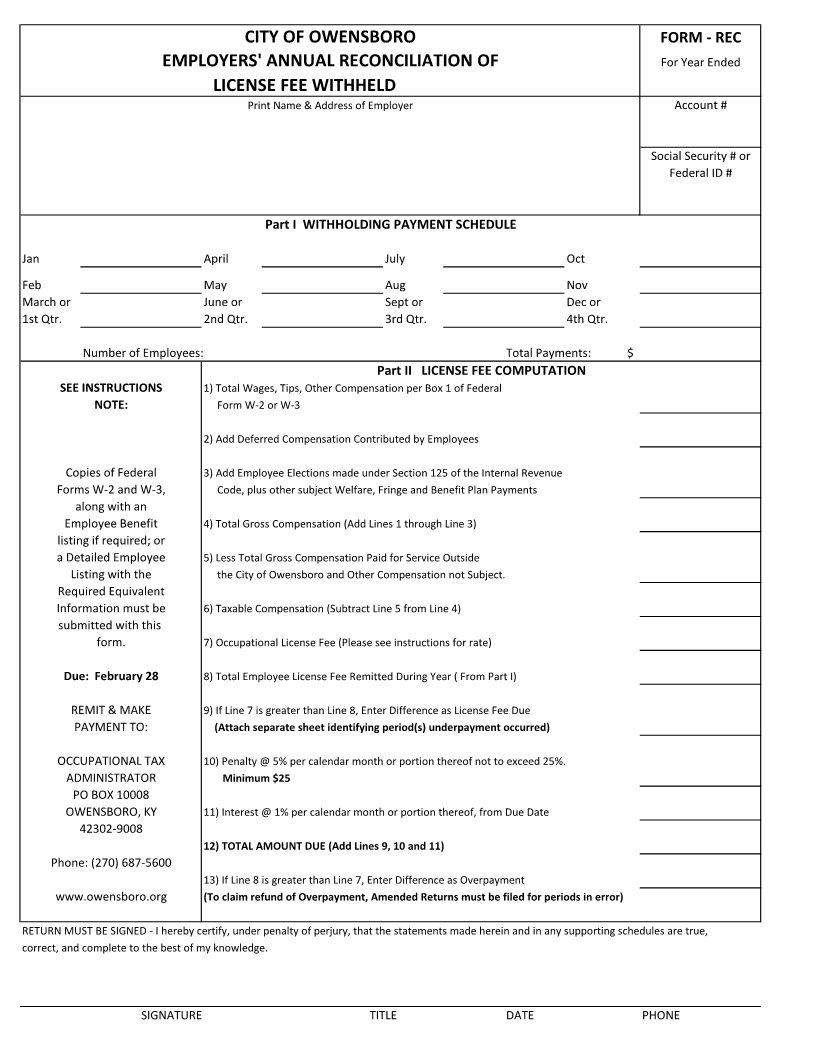
CITY OF OWENSBORO FORM - REC
EMPLOYERS' ANNUAL RECONCILIATION OF For Year Ended
LICENSE FEE WITHHELD
Print Name & Address of Employer Account #
Social Security # or
Federal ID #
Part I WITHHOLDING PAYMENT SCHEDULE
Jan April July Oct
Feb May Aug Nov
March or June or Sept or Dec or
1st Qtr. 2nd Qtr. 3rd Qtr. 4th Qtr.
Number of Employees: Total Payments: $
Part II LICENSE FEE COMPUTATION
SEE INSTRUCTIONS 1)Total Wages, Tips, Other Compensation per Box 1 of Federal
NOTE: Form W-2 or W-3
2)Add Deferred Compensation Contributed by Employees
Copies of Federal 3)Add Employee Elections made under Section 125 of the Internal Revenue
Forms W-2 and W-3, Code, plus other subject Welfare, Fringe and Benefit Plan Payments
along with an
Employee Benefit 4)Total Gross Compensation (Add Lines 1 through Line 3)
listing if required; or
a Detailed Employee 5)Less Total Gross Compensation Paid for Service Outside
Listing with the the City of Owensboro and Other Compensation not Subject.
Required Equivalent
Information must be 6)Taxable Compensation (Subtract Line 5 from Line 4)
submitted with this
form. 7)Occupational License Fee (Please see instructions for rate)
Due: February 28 8)Total Employee License Fee Remitted During Year ( From Part I)
REMIT & MAKE 9)If Line 7 is greater than Line 8, Enter Difference as License Fee Due
PAYMENT TO: (Attach separate sheet identifying period(s) underpayment occurred)
OCCUPATIONAL TAX 10)Penalty @ 5% per calendar month or portion thereof not to exceed 25%.
ADMINISTRATOR Minimum $25
PO BOX 10008
OWENSBORO, KY 11)Interest @ 1% per calendar month or portion thereof, from Due Date
42302-9008
12)TOTAL AMOUNT DUE (Add Lines 9, 10 and 11)
Phone: (270) 687-5600
13)If Line 8 is greater than Line 7, Enter Difference as Overpayment
www.owensboro.org (To claim refund of Overpayment, Amended Returns must be filed for periods in error)
RETURN MUST BE SIGNED - I hereby certify, under penalty of perjury, that the statements made herein and in any supporting schedules are true,
correct, and complete to the best of my knowledge.
SIGNATURE TITLE DATE PHONE