Enlarge image
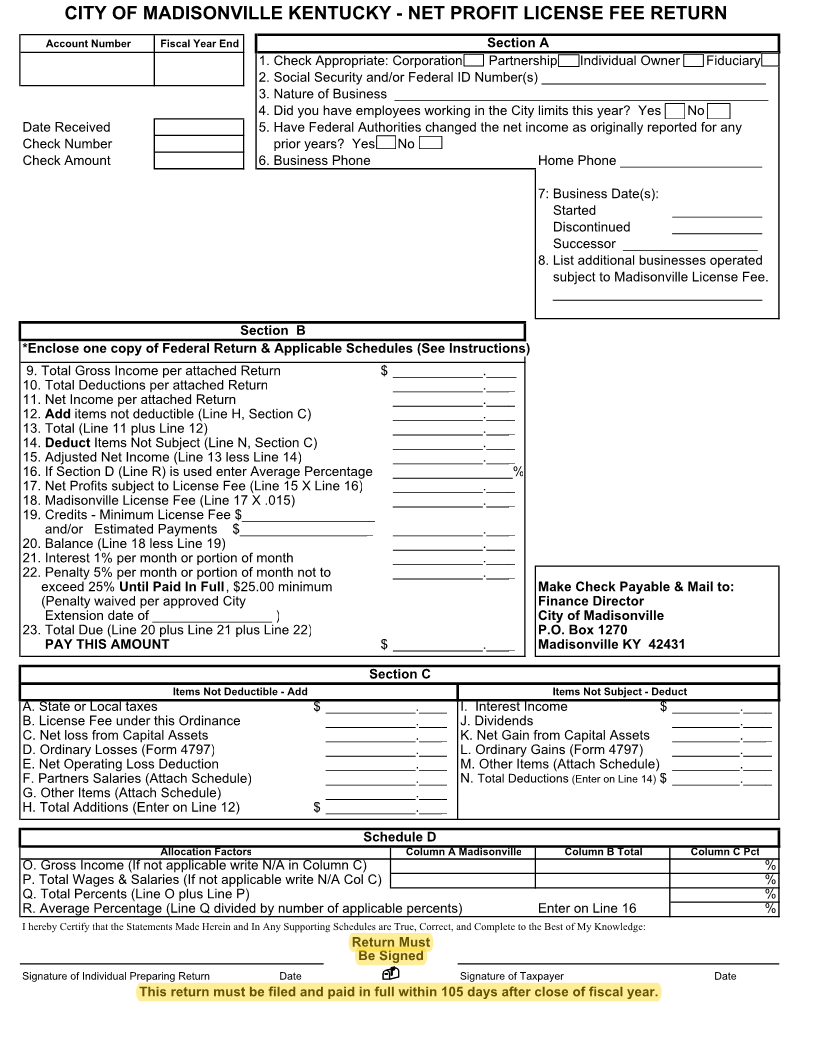
CITY OF MADISONVILLE KENTUCKY - NET PROFIT LICENSE FEE RETURN
Account Number Fiscal Year End Section A
1. Check Appropriate: Corporation Partnership Individual Owner Fiduciary
2. Social Security and/or Federal ID Number(s) ______________________________
3. Nature of Business __________________________________________________
4. Did you have employees working in the City limits this year? Yes No
Date Received 5. Have Federal Authorities changed the net income as originally reported for any
Check Number prior years? Yes No
Check Amount 6.Business Phone Home Phone ___________________
7: Business Date(s):
Started ____________
Discontinued ____________
Successor __________________
8.List additional businesses operated
subject to Madisonville License Fee.
____________________________
Section B
*Enclose one copy of Federal Return & Applicable Schedules (See Instructions)
9.Total Gross Income per attached Return $ ____________.____
10.Total Deductions per attached Return ____________.____
11.Net Income per attached Return ____________.____
12. Add items not deductible (Line H, Section C) ____________.____
13.Total (Line 11 plus Line 12) ____________.____
14. Deduct Items Not Subject (Line N, Section C) ____________.____
15.Adjusted Net Income (Line 13 less Line 14) ____________.____
16.If Section D (Line R) is used enter Average Percentage ________________%
17.Net Profits subject to License Fee (Line 15 X Line 16) ____________.____
18.Madisonville License Fee (Line 17 X .015) ____________.____
19.Credits - Minimum License Fee $__________________
and/or Estimated Payments $__________________ ____________.____
20.Balance (Line 18 less Line 19) ____________.____
21.Interest 1% per month or portion of month ____________.____
22.Penalty 5% per month or portion of month not to ____________.____
exceed 25% Until Paid In Full , $25.00 minimum Make Check Payable & Mail to:
(Penalty waived per approved City Finance Director
Extension date of ________________ ) City of Madisonville
23.Total Due (Line 20 plus Line 21 plus Line 22) P.O. Box 1270
PAY THIS AMOUNT $ ____________.____ Madisonville KY 42431
Section C
Items Not Deductible - Add Items Not Subject - Deduct
A.State or Local taxes $ ____________.____ I. Interest Income $ _________.____
B.License Fee under this Ordinance ____________.____ J.Dividends _________.____
C.Net loss from Capital Assets ____________.____ K.Net Gain from Capital Assets _________.____
D.Ordinary Losses (Form 4797) ____________.____ L.Ordinary Gains (Form 4797) _________.____
E.Net Operating Loss Deduction ____________.____ M.Other Items (Attach Schedule) _________.____
F.Partners Salaries (Attach Schedule) ____________.____ N. Total Deductions (Enter on Line 14) $ _________.____
G.Other Items (Attach Schedule) ____________.____
H.Total Additions (Enter on Line 12) $ ____________.____
Schedule D
Allocation Factors Column A Madisonville Column B Total Column C Pct
O.Gross Income (If not applicable write N/A in Column C) %
P.Total Wages & Salaries (If not applicable write N/A Col C) %
Q.Total Percents (Line O plus Line P) %
R.Average Percentage (Line Q divided by number of applicable percents) Enter on Line 16 %
I hereby Certify that the Statements Made Herein and In Any Supporting Schedules are True, Correct, and Complete to the Best of My Knowledge:
Return Must
Be Signed
Signature of Individual Preparing Return Date Signature of Taxpayer Date
This return must be filed and paid in full within 105 days after close of fiscal year.