Enlarge image
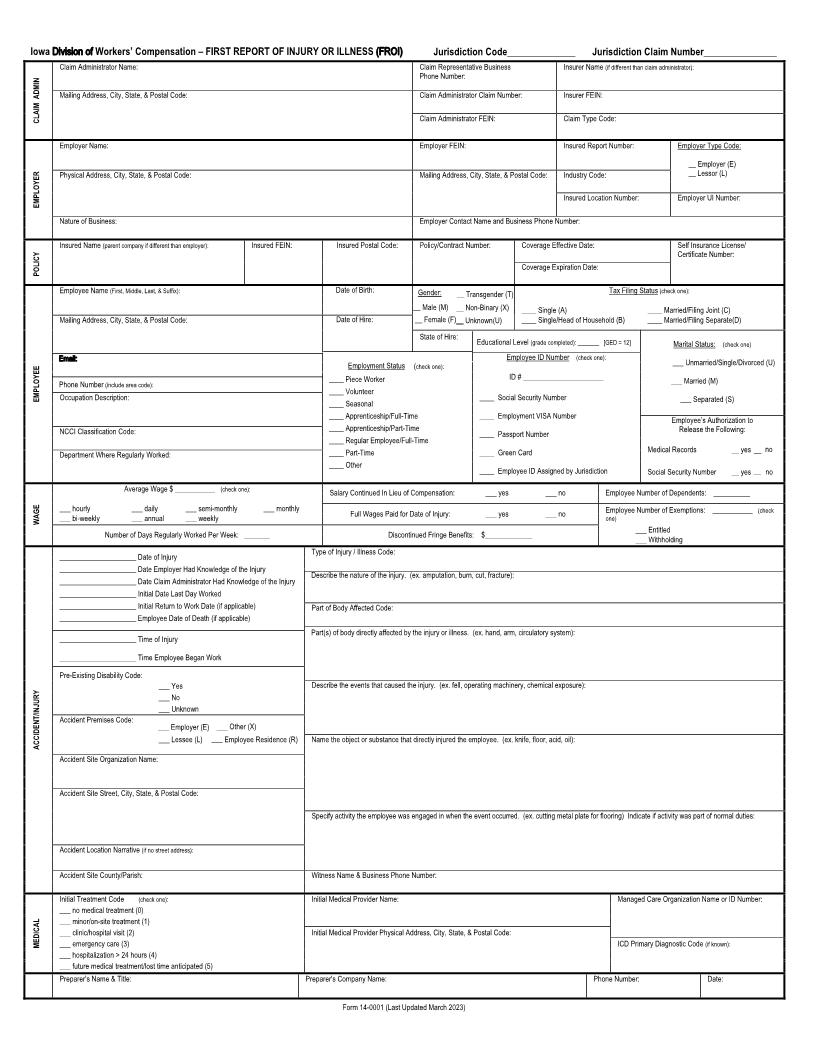
Iowa Division of Workers’ Compensation – FIRST REPORT OF INJURY OR ILLNESS (FROI) Jurisdiction Code______________ Jurisdiction Claim Number_______________
Claim Administrator Name: Claim Representative Business Insurer Name (if different than claim administrator):
Phone Number:
Mailing Address, City, State, & Postal Code: Claim Administrator Claim Number: Insurer FEIN:
CLAIM ADMIN Claim Administrator FEIN: Claim Type Code:
Employer Name: Employer FEIN: Insured Report Number: Employer Type Code:
__ Employer (E)
Physical Address, City, State, & Postal Code: Mailing Address, City, State, & Postal Code: Industry Code: __ Lessor (L)
EMPLOYER Insured Location Number: Employer UI Number:
Nature of Business: Employer Contact Name and Business Phone Number:
Insured Name (parent company if different than employer): Insured FEIN: Insured Postal Code: Policy/Contract Number: Coverage Effective Date: Self Insurance License/
Certificate Number:
POLICY Coverage Expiration Date:
Employee Name (First, Middle, Last, & Suffix): Date of Birth: Gender: __ Transgender (T) Tax Filing Status (check one):
__ Male (M) __ Non-Binary (X) ____ Single (A) ____ Married/Filing Joint (C)
Mailing Address, City, State, & Postal Code: Date of Hire: __ Female (F) Unknown(U)____ ____ Single/Head of Household (B) ____ Married/Filing Separate(D)
State of Hire: Educational Level (grade completed): _______ [GED = 12] Marital Status: (check one)
Employee ID Number (check one):
Email: Employment Status (check one): ___ Unmarried/Single/Divorced (U)
____ Piece Worker ID # ______________________ ___ Married (M)
Phone Number (include area code):
EMPLOYEE Occupation Description: ____ Volunteer ____ Social Security Number ___ Separated (S)
____ Seasonal
____ Apprenticeship/Full-Time ____ Employment VISA Number Employee’s Authorization to
NCCI Classification Code: ____ Apprenticeship/Part-Time ____ Passport Number Release the Following:
____ Regular Employee/Full-Time
Department Where Regularly Worked: ____ Part-Time ____ Green Card Medical Records __ yes __ no
____ Other ____ Employee ID Assigned by Jurisdiction Social Security Number __ yes __ no
Average Wage $ ___________ (check one): Salary Continued In Lieu of Compensation: ___ yes ___ no Employee Number of Dependents: __________
___ hourly ___ daily ___ semi-monthly ___ monthly Full Wages Paid for Date of Injury: ___ yes ___ no Employee Number of Exemptions: ___________ (check
WAGE ___ bi-weekly ___ annual ___ weekly one)
Number of Days Regularly Worked Per Week: _______ Discontinued Fringe Benefits: $_____________ ___ Entitled___ Withholding
_____________________ Date of Injury Type of Injury / Illness Code:
_____________________ Date Employer Had Knowledge of the Injury Describe the nature of the injury. (ex. amputation, burn, cut, fracture):
_____________________ Date Claim Administrator Had Knowledge of the Injury
_____________________ Initial Date Last Day Worked
_____________________ Initial Return to Work Date (if applicable) Part of Body Affected Code:
_____________________ Employee Date of Death (if applicable)
Part(s) of body directly affected by the injury or illness. (ex. hand, arm, circulatory system):
_____________________ Time of Injury
_____________________ Time Employee Began Work
Pre-Existing Disability Code:
___ Yes Describe the events that caused the injury. (ex. fell, operating machinery, chemical exposure):
___ No
___ Unknown
Accident Premises Code:
___ Employer (E) ___ Other (X)
ACCIDENT/INJURY ___ Lessee (L) ___ Employee Residence R( ) Name the object or substance that directly injured the employee. (ex. knife, floor, acid, oil):
Accident Site Organization Name:
Accident Site Street, City, State, & Postal Code:
Specify activity the employee was engaged in when the event occurred. (ex. cutting metal plate for flooring) Indicate if activity was part of normal duties:
Accident Location Narrative (if no street address):
Accident Site County/Parish: Witness Name & Business Phone Number:
Initial Treatment Code (check one): Initial Medical Provider Name: Managed Care Organization Name or ID Number:
___ no medical treatment (0)
___ minor/on-site treatment (1)
___ clinic/hospital visit (2) Initial Medical Provider Physical Address, City, State, & Postal Code:
MEDICAL ___ emergency care (3) ICD Primary Diagnostic Code (if known):
___ hospitalization > 24 hours (4)
___ future medical treatment/lost time anticipated (5)
Preparer’s Name & Title: Preparer's Company Name: Phone Number: Date:
Form 14-0001 (Last Updated March 2023)