Enlarge image
Power of Attorney Declaration
This Power of Attorney (POA) Declaration (DE 48) is your written authorization for an individual or other entity to act on your
behalf in tax and/or benefit reporting matters with us. A POA remains in effect until it is revoked or a new one is received.
If you would like to only authorize a POA for a set period, you must specify the date your new POA will expire.
For more information, see the Information Sheet: Counseling Service Agent (DE 231CSA) and Information Sheet: Payroll
Reporting Agent (DE 231PRA).
Complete the DE 48
Online
Complete and send us your POA online with e-Services for Business (eddservices.edd.ca.gov/tap/secure/eservices).
For more information, visit e-Services for Business FAQs (edd.ca.gov/en/payroll_taxes/faq_-_e-services_for_business).
By Mail
You can also send a POA by mailing the completed DE 48 with the following required information:
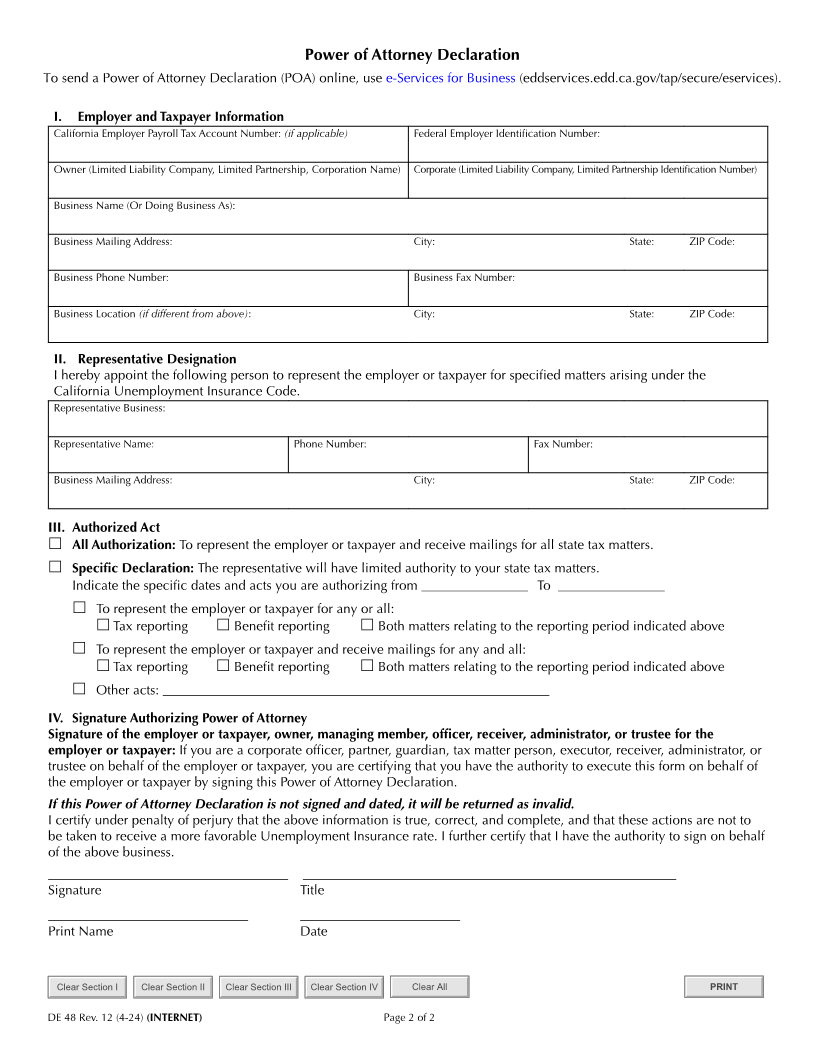
Employer and taxpayer information
Enter your:
• California employer payroll tax account number (if applicable)
• Federal employer identification number
• Owner or legal name of organization
• Secretary of State identification number
• Business name or doing business (DBA)
• Mailing address
• Business phone and fax numbers
• Business location if different than the mailing address
Representative designation
Enter your representative’s business, name, phone number, fax numbers and address.
• Authorized acts
If you want to authorize your representative to perform all acts on your behalf, select the General Authorization
box.
• If you want to limit this authorization, select the boxes that apply under the “Specific Declaration” header.
Enter the beginning and ending dates of each interval or period you are making the declaration.
Signature authorizing power of attorney
In order for your new POA to be recognized, it must be signed and dated by an authorized signator.
An authorized signator can be the business:
• Owner
• Partners
• Members
• Managing members
• Corporate officers including the President, Vice President, Chief Executive Officer, or Chief Financial Officer
Please send an updated list of corporate officers or owners with this document.
Note: If your declaration is sent without a date, signature, or with an unauthorized signature, it will be returned.
The signature date must be within 30 days of the submission of the POA.
Mail the completed DE 48 to:
Employment Development Department
Account Services Group, MIC 28
PO Box 826880
Sacramento, CA 94280-0001
Fax 1-916-654-9211
Questions or need assistance completing this form? Call the Account Services Group Agent Line at 1-916-654-7263.
DE 48 Rev. 12 (4-2 )4 (INTERNET) Page 1 of 2 CU