Enlarge image
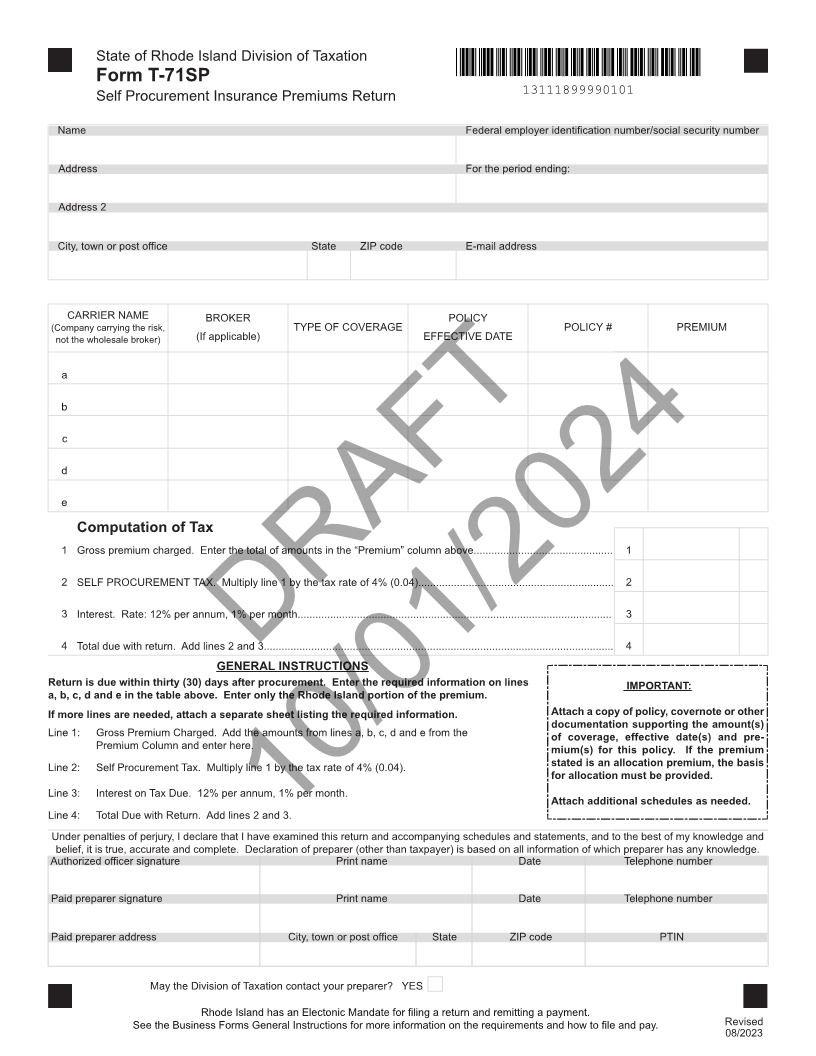
State of Rhode Island Division of Taxation
Form T-71SP
Self Procurement Insurance Premiums Return 13111899990101
Name Federal employer identification number/social security number
Address For the period ending:
Address 2
City, town or post office State ZIP code E-mail address
CARRIER NAME BROKER POLICY
(Company carrying the risk, TYPE OF COVERAGE POLICY # PREMIUM
not the wholesale broker) (If applicable) EFFECTIVE DATE
a
b
c
d
e
Computation of Tax
1 Gross premium charged. Enter the total of amounts in the “Premium” column above............................................... 1
2 SELF PROCUREMENT TAX. Multiply line 1 by the tax rate of 4% (0.04).................................................................. 2
3 Interest. Rate: 12% per annum, 1% per month.......................................................................................................... 3
4 Total due with return. Add lines 2 and 3...................................................................................................................... 4
GENERAL INSTRUCTIONSDRAFT
Return is due within thirty (30) days after procurement. Enter the required information on lines IMPORTANT:
a, b, c, d and e in the table above. Enter only the Rhode Island portion of the premium.
Attach a copy of policy, covernote or other
If more lines are needed, attach a separate sheet listing the required information. documentation supporting the amount(s)
Line 1: Gross Premium Charged. Add the amounts from lines a, b, c, d and e from the of coverage, effective date(s) and pre-
Premium Column and enter here. mium(s) for this policy. If the premium
Line 2: Self Procurement Tax. Multiply line 1 by the tax rate of 4% (0.04). stated is an allocation premium, the basis
for allocation must be provided.
Line 3: Interest on Tax Due. 12% per annum, 1% per month.
Attach additional schedules as needed.
Line 4: Total Due with Return. Add lines 2 and 3.
Under penalties of perjury, I declare that I have examined10/01/2024this return and accompanying schedules and statements, and to the best of my knowledge and
belief, it is true, accurate and complete. Declaration of preparer (other than taxpayer) is based on all information of which preparer has any knowledge.
Authorized officer signature Print name Date Telephone number
Paid preparer signature Print name Date Telephone number
Paid preparer address City, town or post office State ZIP code PTIN
May the Division of Taxation contact your preparer? YES
Rhode Island has an Electonic Mandate for filing a return and remitting a payment.
See the Business Forms General Instructions for more information on the requirements and how to file and pay. Revised
08/2023