Enlarge image
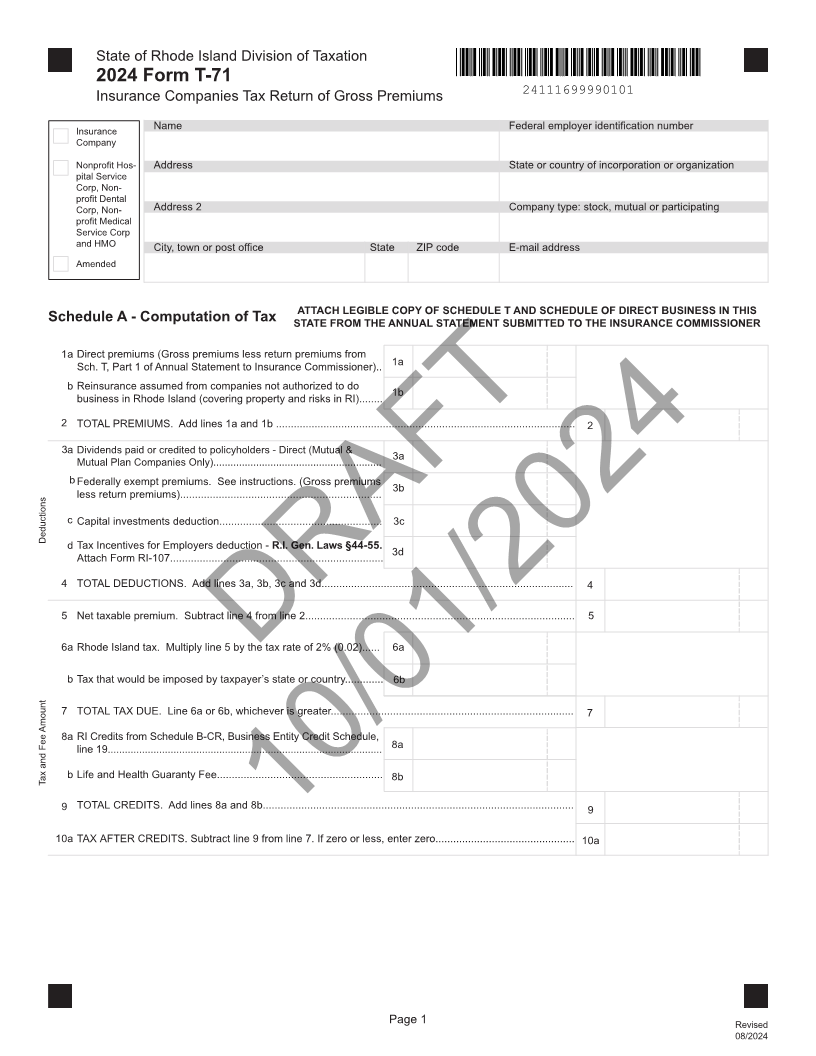
State of Rhode Island Division of Taxation 2024 Form T-71 Insurance Companies Tax Return of Gross Premiums 24111699990101 Insurance Name Federal employer identification number Company Nonprofit Hos- Address State or country of incorporation or organization pital Service Corp, Non- profit Dental Corp, Non- Address 2 Company type: stock, mutual or participating profit Medical Service Corp and HMO City, town or post office State ZIP code E-mail address Amended ATTACH LEGIBLE COPY OF SCHEDULE T AND SCHEDULE OF DIRECT BUSINESS IN THIS Schedule A - Computation of Tax STATE FROM THE ANNUAL STATEMENT SUBMITTED TO THE INSURANCE COMMISSIONER 1 a Direct premiums (Gross premiums less return premiums from Sch. T, Part 1 of Annual Statement to Insurance Commissioner).. 1a b Reinsurance assumed from companies not authorized to do 1b business in Rhode Island (covering property and risks in RI)........ 2 TOTAL PREMIUMS. Add lines 1a and 1b ..................................................................................................... 2 3 a Dividends paid or credited to policyholders - Direct (Mutual & 3a Mutual Plan Companies Only)........................................................... b Federally exempt premiums. See instructions. (Gross premiums 3b less return premiums).................................................................... c Capital investments deduction....................................................... 3c Deductions d Tax Incentives for Employers deduction - R.I. Gen. Laws §44-55. 3d Attach Form RI-107........................................................................ 4 TOTAL DEDUCTIONS. Add lines 3a, 3b, 3c and 3d..................................................................................... 4 5 Net taxable premium. Subtract line 4 from line 2........................................................................................... 5 6a Rhode Island tax. Multiply line 5 by the tax rate of 2% (0.02)...... 6a DRAFT b Tax that would be imposed by taxpayer’s state or country............. 6b 7 TOTAL TAX DUE. Line 6a or 6b, whichever is greater.................................................................................. 7 8 a RI Credits from Schedule B-CR, Business Entity Credit Schedule, line 19................................................................................................ 8a Tax and Fee Amount b Life and Health Guaranty Fee........................................................ 8b 9 TOTAL CREDITS. Add lines 8a and 8b......................................................................................................... 9 10aTAX AFTER CREDITS. Subtract line 9 from line 7.10/01/2024If zero or less, enter zero...............................................10a Page 1 Revised 08/2024