Enlarge image
Clear Form
STATE OF HAWAII—DEPARTMENT OF TAXATION THIS SPACE FOR DATE RECEIVED STAMP
FORM
EXEMPT ORGANIZATION BUSINESS
N-70NP
(REV. 2023) INCOME TAX RETURN
For calendar year
2023
or other taxable year beginning _______________________, 2023
and ending _______________________, 20____
N70NP_I 2023A 01 VID01 Final Return Amended Return (Attach Sch AMD) IRS Adjustment NOL Carryback
Name of organization A Federal Employer I.D. No.
Dba or C/O B Unrelated business activity code(s)
Mailing Address (number and street) C Hawaii Tax I.D. No.
PRINT OR TYPE City or town, State and Postal/ZIP code. If this is a foreign address, see Instructions. D This organization is a (check one):
Corporation Charitable Trust
ENTER APPROPRIATE AMOUNTS FROM FEDERAL FORM 990-T. Note: The sum of lines 1 - 5 DO NOT equal line 6.
1 Gross receipts or sales . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2 Returns and allowances . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
3 Cost of goods sold and/or operations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
4 Capital gain net income (see Instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
5 Other income . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Taxable Income 6 Total unrelated trade or business income. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
7 Total deductions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
8 Unrelated business taxable income . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
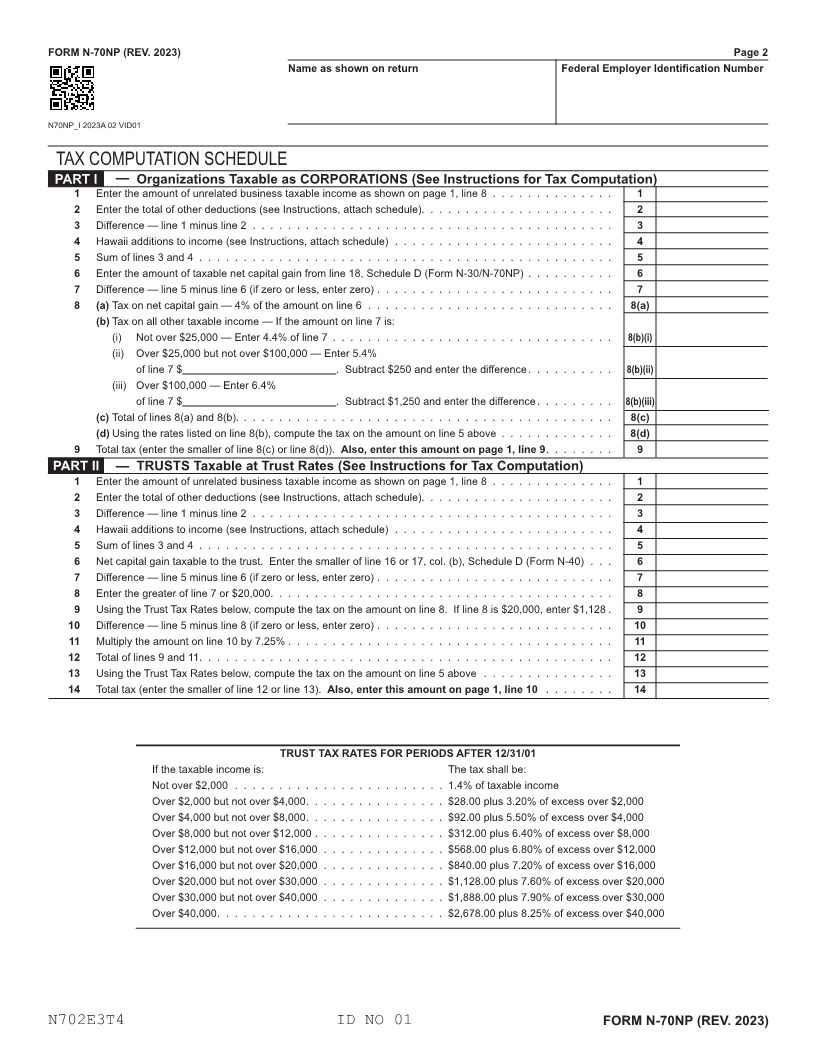
9 Tax — From TAX COMPUTATION SCHEDULE on page 2, Part I, line 9 . . . . . . . . . . . . . . . . . . . 9
10 Tax — From TAX COMPUTATION SCHEDULE on page 2, Part II, line 14 . . . . . . . . . . . . . . . . . . 10
11 Recapture of Capital Goods Excise Tax Credit from Form N-312, Part II (attach Form N-312) . . . . . . . . . 11
12 Recapture of Low-Income Housing Tax Credit from Form N-586, Part III (attach Form N-586) . . . . . . . . . 12
13 Recapture of Tax Credit for Flood Victims from Form N-338 (attach Form N-338) . . . . . . . . . . . . . . . . 13
14Tax ComputationRecapture of Important Agricultural Land Qualified Agricultural Cost Tax Credit (attach Form N-344) . . . . . . 14
15 Recapture of Capital Infrastructure Tax Credit (attach Form N-348) . . . . . . . . . . . . . . . . . . . . . . . 15
16 Total tax (add lines 9 or 10 and 11, 12, 13, 14, and 15) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
17 Total refundable tax credits from Schedule CR, line 10 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
18 ADJUSTED TAX LIABILITYLine— 16 minus line 17. If line 18 is zero or less, see Instructions. . . . . . . . 18
19 Total nonrefundable credits from Schedule CR, line 32 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
20 Line 18 minus line 19 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
21 Credits and payments:
(a) 2022 overpayment credited to 2023 . . . . . . . . . . . . . . . . . . . . . 21(a) ATTACH COPY OF
(b) Estimated tax payments. . . . . . . . . . . . . . . . . . . . . . . . . . . . 21(b) FEDERAL FORM
(c) Tax paid with automatic extension of time to file . . . . . . . . . . . . . . . 21(c) 990-T
(d) Total credits and payments (add lines 21(a) through 21(c)). . . . . . . . . . . . . . . . . . . . . . . . . . 21(d)
Total Income Tax 22 Estimated tax penalty (see Instructions). Check if Form N-220 is attached . . . . . . . . . . . . . . . . 22
ATTACH CHECK OR MONEY ORDER HERE 23 TAX DUE — If line 21(d) is smaller than the total of lines 20 and 22, enter amount owed (see Instructions) . . 23
24 OVERPAYMENT — If line 21(d) is larger than the total of lines 20 and 22, enter amount overpaid (see Instructions) . . . 24
25 (a) Enter the amount of line 24 you want Credited to 2024 estimated tax . . . . . . . . . . . . . . . . . . 25(a)
(b) Enter the amount of line 24 you want Refunded to you (line 24 minus line 25(a)) . . . . . . . . . . . . 25(b)
26 Enter AMOUNT PAID with this return . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
27 Amount paid (overpaid) on original return — AMENDED RETURN ONLY (see Instructions) . . . . . . . . . . 27
Amended Return 28 BALANCE DUE (REFUND) with amended return (see Instructions) . . . . . . . . . . . . . . . . . . . . . . . 28
I declare, under the penalties set forth in section 231-36, HRS, that this return (including any accompanying schedules or statements) has been examined by me and, to the best of my knowledge
and belief, is true, correct, and complete. Declaration of preparer (other than taxpayer) is based on all information of which preparer has any knowledge.
Signature of officer Date Name and title of officer
May the Hawaii Department of Taxation discuss this return with the preparer shown below? (See page 5 of the Instructions) Yes No
This designation does not replace Form N-848, Power of Attorney.
Preparer’s signature Date Check if PTIN
Paid Print Preparer’s Name self-employed
Please Sign Here Preparer’s
E.I. No
Information Firm’s name (or yours, Federal
ifAddressself-employed)and ZIP Code Phone. no.
N701E3T4 ID NO 01 FORM N-70NP (REV. 2023)