Enlarge image
Clear Form
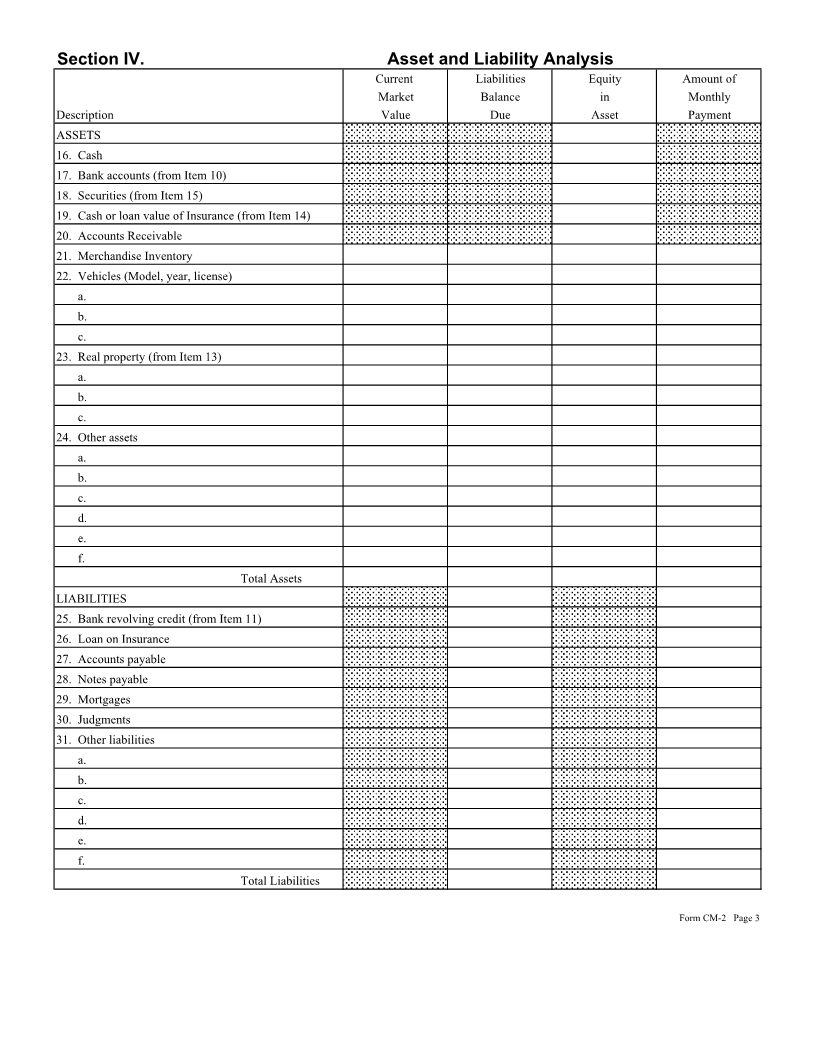
Form CM - 2 Department of Taxation - State of Hawaii
(Rev. 2018)
STATEMENT OF FINANCIAL CONDITION AND OTHER INFORMATION
Section I. General Information - For Individuals
1. Taxpayer(s) name(s) and address 2. Home phone no. 3. Marital status
4a. Taxpayer's social security no. b. Spouse's social security no.
5a. Taxpayer's birth date b. Spouse's birth date 6. Other names or aliases
7. Name, age, social security number, and relationship of dependents living in your household.
Section II. Employment Information
8. Taxpayer's employer or business a. How long employed? b. Business phone no. c. Occupation
(name and address)
d. Check appropriate item
( ) Wage earner ( ) Sole proprietor ( ) Partner
9. Spouse's employer or business a. How long employed? c. Business phone no. c. Occupation
(name and address)
d. Check appropriate item
( ) Wage earner ( ) Sole proprietor ( ) Partner
Section III. General Financial Information
10. Bank accounts (include Savings & Loans, Credit Unions, IRA and Retirment Plans, Certificate of Deposits, etc.)
Attach additional sheets as necessary.
Name of Institution Address Type of Account Account No. Balance
Total (Enter in Item 17)
CM2_I 2018A 01 VID01 ID NO 01 Form CM-2 Page 1Form CM-2 Page 1