Enlarge image
OMB No. 1545-0074
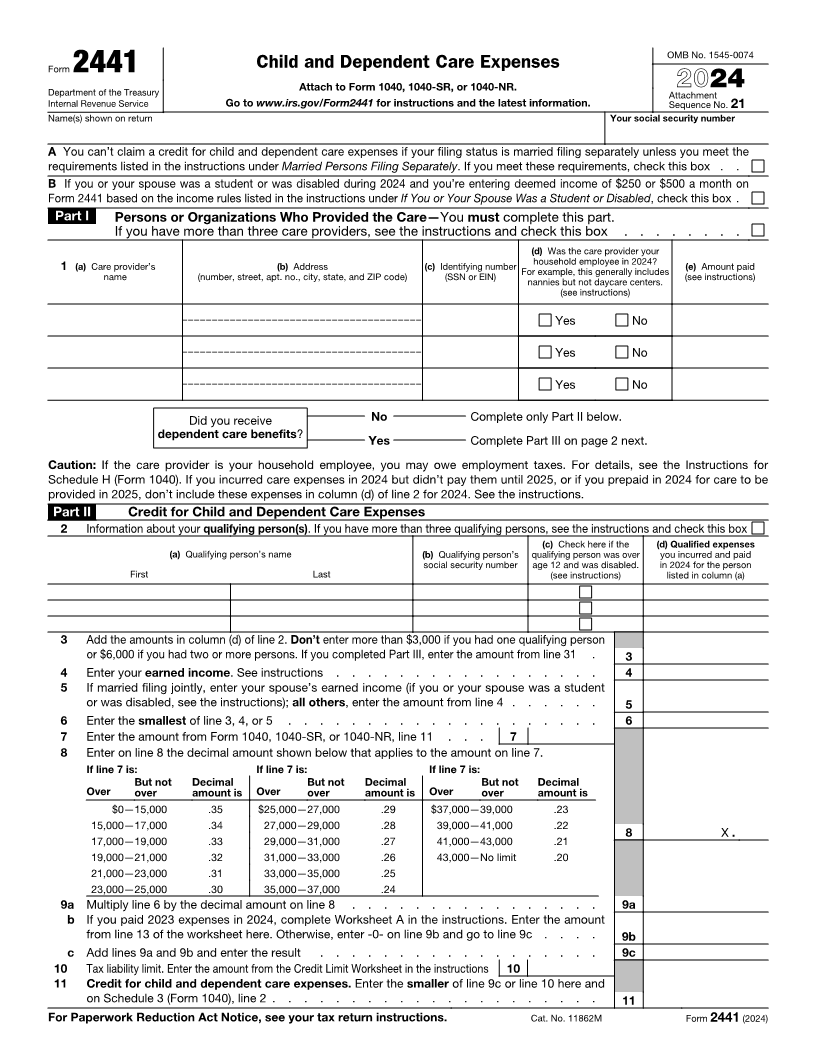
Child and Dependent Care Expenses
Form 2441
Department of the Treasury Attach to Form 1040, 1040-SR, or 1040-NR. 2024
Attachment
Internal Revenue Service Go to www.irs.gov/Form2441 for instructions and the latest information. Sequence No. 21
Name(s) shown on return Your social security number
A You can’t claim a credit for child and dependent care expenses if your filing status is married filing separately unless you meet the
requirements listed in the instructions under Married Persons Filing Separately. If you meet these requirements, check this box . .
B If you or your spouse was a student or was disabled during 2024 and you’re entering deemed income of $250 or $500 a month on
Form 2441 based on the income rules listed in the instructions under If You or Your Spouse Was a Student or Disabled, check this box .
Part I Persons or Organizations Who Provided the Care—You must complete this part.
If you have more than three care providers, see the instructions and check this box . . . . . . . .
(d) Was the care provider your
1 (a) Care provider’s (b) Address (c) Identifying number household employee in 2024? (e) Amount paid
name (number, street, apt. no., city, state, and ZIP code) (SSN or EIN) For example, this generally includes (see instructions)
nannies but not daycare centers.
(see instructions)
Yes No
Yes No
Yes No
Did you receive No Complete only Part II below.
dependent care benefits?
Yes Complete Part III on page 2 next.
Caution: If the care provider is your household employee, you may owe employment taxes. For details, see the Instructions for
Schedule H (Form 1040). If you incurred care expenses in 2024 but didn’t pay them until 2025, or if you prepaid in 2024 for care to be
provided in 2025, don’t include these expenses in column (d) of line 2 for 2024. See the instructions.
Part II Credit for Child and Dependent Care Expenses
2 Information about your qualifying person(s). If you have more than three qualifying persons, see the instructions and check this box
(c) Check here if the (d) Qualified expenses
(a) Qualifying person’s name (b) Qualifying person’s qualifying person was over you incurred and paid
social security number age 12 and was disabled. in 2024 for the person
First Last (see instructions) listed in column (a)
3 Add the amounts in column (d) of line 2. Don’t enter more than $3,000 if you had one qualifying person
or $6,000 if you had two or more persons. If you completed Part III, enter the amount from line 31 . 3
4 Enter your earned income. See instructions . . . . . . . . . . . . . . . . . 4
5 If married filing jointly, enter your spouse’s earned income (if you or your spouse was a student
or was disabled, see the instructions); all others, enter the amount from line 4 . . . . . . 5
6 Enter the smallest of line 3, 4, or 5 . . . . . . . . . . . . . . . . . . . . 6
7 Enter the amount from Form 1040, 1040-SR, or 1040-NR, line 11 . . . 7
8 Enter on line 8 the decimal amount shown below that applies to the amount on line 7.
If line 7 is: If line 7 is: If line 7 is:
But not Decimal But not Decimal But not Decimal
Over over amount is Over over amount is Over over amount is
$0—15,000 .35 $25,000—27,000 .29 $37,000—39,000 .23
15,000—17,000 .34 27,000—29,000 .28 39,000—41,000 .22
8 X .
17,000—19,000 .33 29,000—31,000 .27 41,000—43,000 .21
19,000—21,000 .32 31,000—33,000 .26 43,000—No limit .20
21,000—23,000 .31 33,000—35,000 .25
23,000—25,000 .30 35,000—37,000 .24
9 a Multiply line 6 by the decimal amount on line 8 . . . . . . . . . . . . . . . . 9a
b If you paid 2023 expenses in 2024, complete Worksheet A in the instructions. Enter the amount
from line 13 of the worksheet here. Otherwise, enter -0- on line 9b and go to line 9c . . . . 9b
c Add lines 9a and 9b and enter the result . . . . . . . . . . . . . . . . . . 9c
10 Tax liability limit. Enter the amount from the Credit Limit Worksheet in the instructions 10
11 Credit for child and dependent care expenses. Enter the smaller of line 9c or line 10 here and
on Schedule 3 (Form 1040), line 2 . . . . . . . . . . . . . . . . . . . . . 11
For Paperwork Reduction Act Notice, see your tax return instructions. Cat. No. 11862M Form 2441 (2024)