Enlarge image
1 1
NEAR FINAL 8/1/24
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56 58 60 62 64 66 68 70 72 74 76 78 80 82 84 86
3 3
4 4
5 5
*226281*
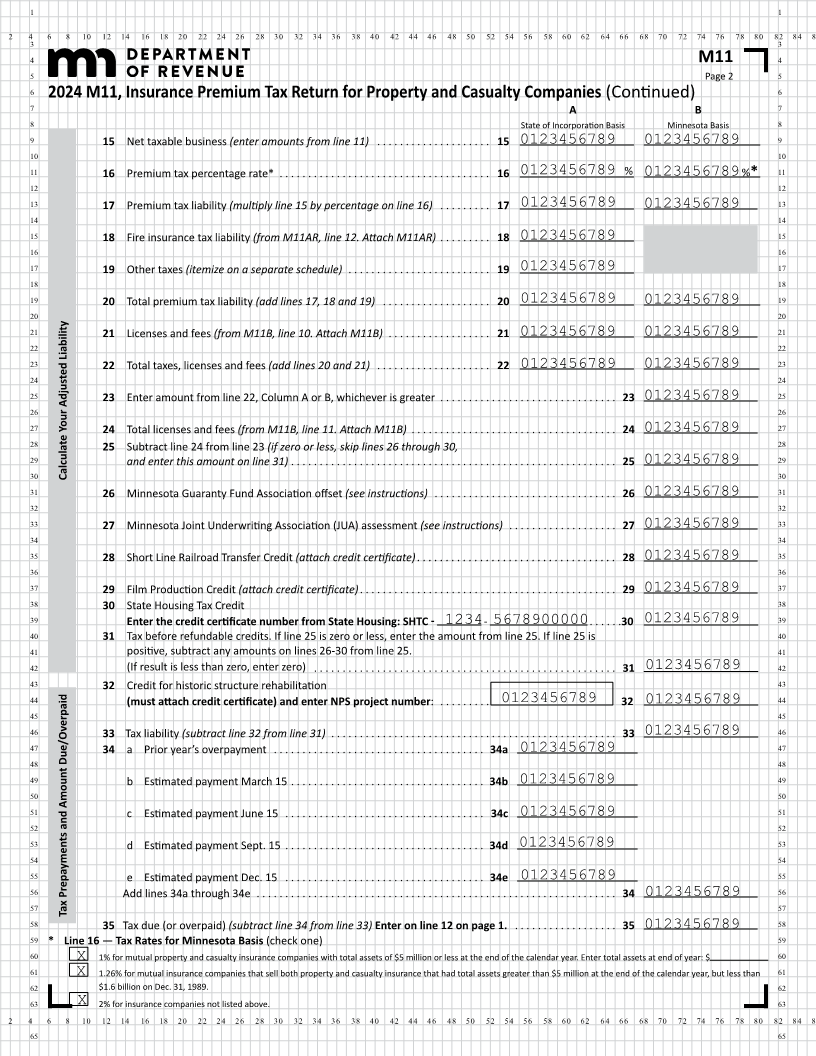
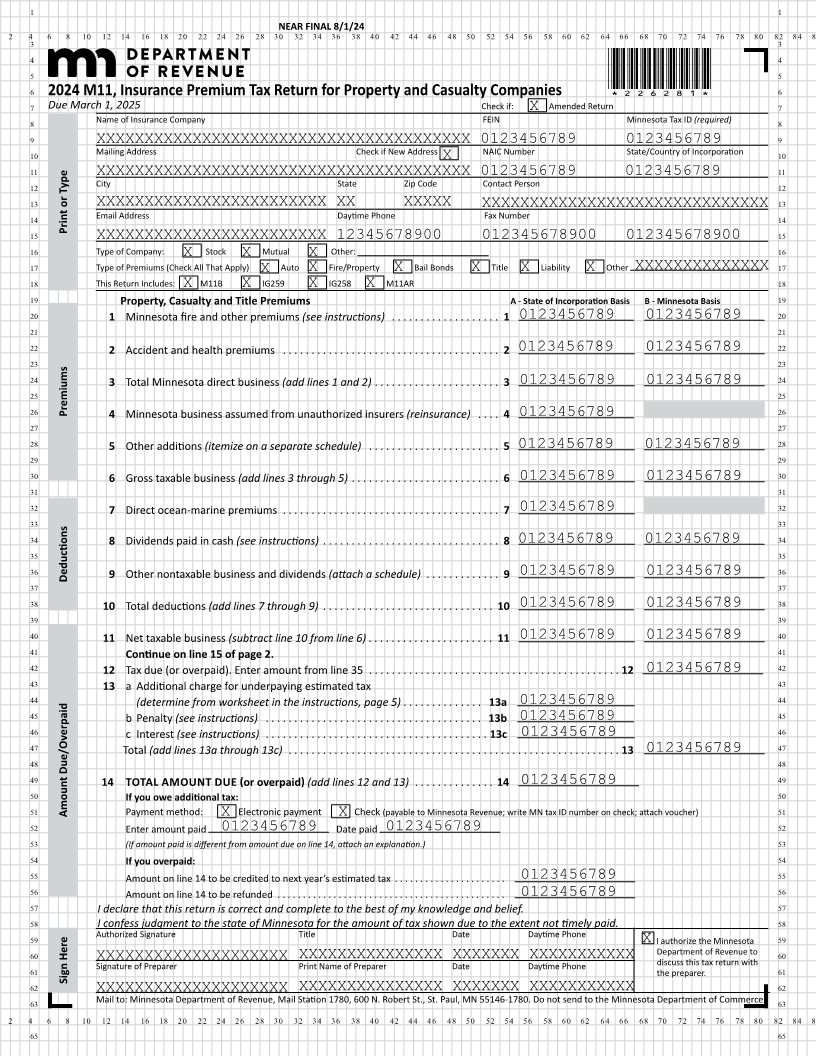
6 2024 M11, Insurance Premium Tax Return for Property and Casualty Companies 6
7 Due March 1, 2025 Check if: Amended Return 7
8 Name of Insurance Company FEIN X Minnesota Tax ID(required) 8
9 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 0123456789 0123456789 9
10 Mailing Address Check if New Address NAIC Number State/Country of Incorporation 10
X
11 XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 0123456789 0123456789 11
12 City State Zip Code Contact Person 12
13 XXXXXXXXXXXXXXXXXXXXXXXX XX XXXXX XXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 13
14 Email Address Daytime Phone Fax Number 14
Print or Type
15 XXXXXXXXXXXXXXXXXXXXXXXX 12345678900 012345678900 012345678900 15
16 Type of Company: Stock Mutual Other: 16
X X X
17 Type of Premiums (Check All That Apply) X Auto X Fire/Property X Bail Bonds X Title X Liability X Other XXXXXXXXXXXXXX 17
18 This Return Includes: X M11B X IG259 X IG258 X M11AR 18
19 Property, Casualty and Title Premiums A - State of Incorporation Basis B - Minnesota Basis 19
20 1 Minnesota fire and other premiums (see instructions) . . . . . . . . . . . . . . . . . . . 1 0123456789 0123456789 20
21 21
22 2 Accident and health premiums . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 0123456789 0123456789 22
23 23
24 3 Total Minnesota direct business (add lines 1 and 2) . . . . . . . . . . . . . . . . . . . . . . 3 0123456789 0123456789 24
25 25
26 Premiums 4 Minnesota business assumed from unauthorized insurers (reinsurance) . . . . 4 26
0123456789
27 27
28 5 Other additions (itemize on a separate schedule) . . . . . . . . . . . . . . . . . . . . . . . 5 0123456789 0123456789 28
29 29
30 6 Gross taxable business (add lines 3 through 5) . . . . . . . . . . . . . . . . . . . . . . . . . . 6 0123456789 0123456789 30
31 31
32 7 Direct ocean-marine premiums . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 0123456789 32
33 33
34 8 Dividends paid in cash (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 0123456789 0123456789 34
35 35
36 Deductions 9 Other nontaxable business and dividends (attach a schedule) . . . . . . . . . . . . . 9 0123456789 0123456789 36
37 37
38 10 Total deductions (add lines 7 through 9) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 0123456789 0123456789 38
39 39
40 11 Net taxable business (subtract line 10 from line 6) . . . . . . . . . . . . . . . . . . . . . . 11 0123456789 0123456789 40
41 Continue on line 15 of page 2. 41
42 12 Tax due (or overpaid) . Enter amount from line 35 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 0123456789 42
43 13 a Additional charge for underpaying estimated tax 43
44 (determine from worksheet in the instructions, page 5) . . . . . . . . . . . . . . 13a 0123456789 44
45 b Penalty (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13b 0123456789 45
46 c Interest (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13c 0123456789 46
47 Total (add lines 13a through 13c) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 0123456789 47
48 48
49 14 TOTAL AMOUNT DUE (or overpaid ) (add lines 12 and 13) . . . . . . . . . . . . . . 14 0123456789 49
50 If you owe additional tax: 50
51 Amount Due/Overpaid Payment method: Electronic payment Check (payable to Minnesota Revenue; write MN tax ID number on check; attach voucher) 51
X X
52 Enter amount paid 0123456789 Date paid 0123456789 52
53 (If amount paid is different from amount due on line 14, attach an explanation.) 53
54 If you overpaid: 54
55 Amount on line 14 to be credited to next year’s estimated tax . . . . . . . . . . . . . . . . . . . . . . 0123456789 55
56 Amount on line 14 to be refunded . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0123456789 56
57 I declare that this return is correct and complete to the best of my knowledge and belief. 57
58 I confess judgment to the state of Minnesota for the amount of tax shown due to the extent not timely paid. 58
59 Authorized Signature Title Date Daytime Phone 59
X I authorize the Minnesota
60 Department of Revenue to 60
61 SignatureXXXXXXXXXXXXXXXXXXXXof Preparer PrintXXXXXXXXXXXXXXXName Preparerof DateXXXXXXXDaytimeXXXXXXXXXXXPhone discuss this tax return with 61
Sign Here the preparer .
62 XXXXXXXXXXXXXXXXXXXX XXXXXXXXXXXXXXX XXXXXXX XXXXXXXXXXX 62
63 Mail to: Minnesota Department of Revenue, Mail Station 1780, 600 N. Robert St., St. Paul, MN 55146-1780. Do not send to the Minnesota Department of Commerce. 63
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56 58 60 62 64 66 68 70 72 74 76 78 80 82 84 86
65 65