Enlarge image
1 1
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56 58 60 62 64 66 68 70 72 74 76 78 80 82 84 86
3 NEAR FINAL DRAFT 8/1/24 3
4 4
5 5
6 *226331* 6
7 7
8 8
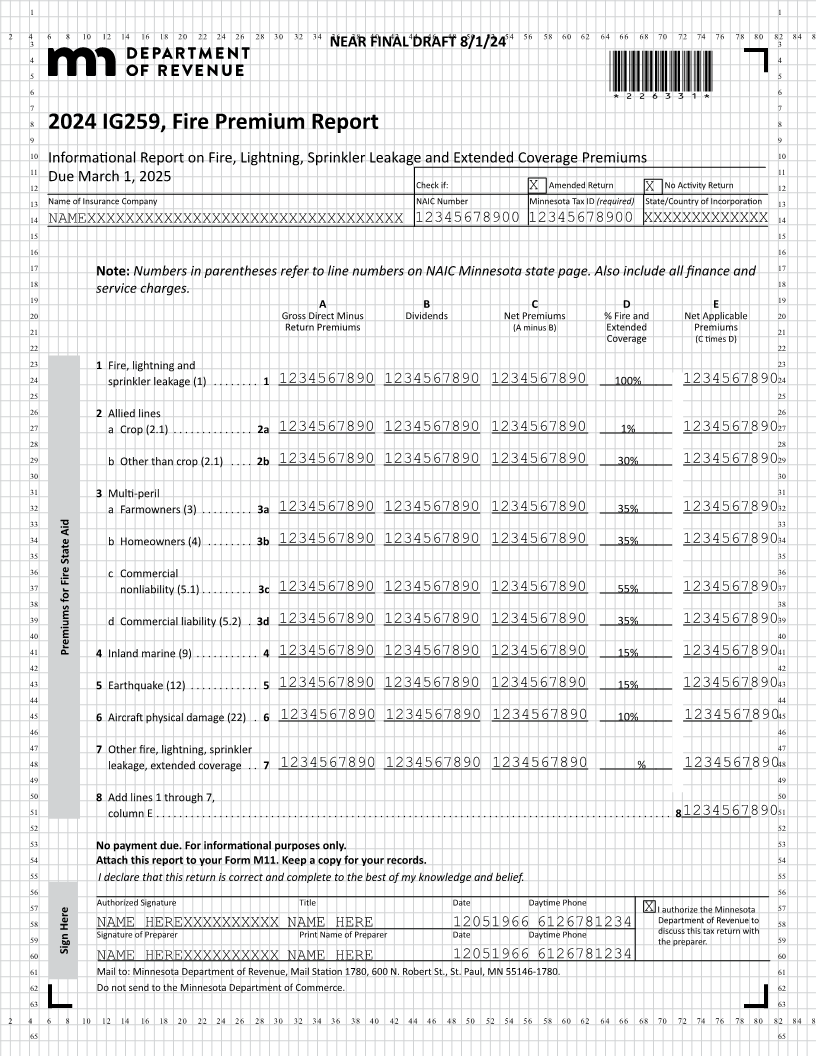
2024 IG259, Fire Premium Report
9 9
10 Informational Report on Fire, Lightning, Sprinkler Leakage and Extended Coverage Premiums 10
11 11
Due March 1, 2025
12 Check if: X Amended Return No Activity Return 12
X
13 Name of Insurance Company NAIC Number Minnesota Tax ID (required) State/Country of Incorporation 13
14 NAMEXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX 12345678900 12345678900 XXXXXXXXXXXXX 14
15 15
16 16
17 Numbers in parentheses refer to line numbers on NAIC Minnesota state page. Also include all finance and 17
Note:
18 18
service charges.
19 A B C D E 19
20 Gross Direct Minus Dividends Net Premiums % Fire and Net Applicable 20
21 Return Premiums (A minus B) Extended Premiums 21
Coverage (C times D)
22 22
23 1 Fire, lightning and 23
24 sprinkler leakage (1) . . . . . . . . 1 1234567890 1234567890 1234567890 100% 123456789024
25 25
26 2 Allied lines 26
27 a Crop (2 .1) . . . . . . . . . . . . . . 2a 1234567890 1234567890 1234567890 1% 123456789027
28 28
29 b Other than crop (2 .1) . . . . 2b 1234567890 1234567890 1234567890 30% 123456789029
30 30
31 3 Multi-peril 31
32 a Farmowners (3) . . . . . . . . . 3a 1234567890 1234567890 1234567890 35% 123456789032
33 33
34 b Homeowners (4) . . . . . . . . 3b 1234567890 1234567890 1234567890 35% 123456789034
35 35
36 c Commercial 36
37 nonliability (5 .1) . . . . . . . . . 3c 1234567890 1234567890 1234567890 55% 123456789037
38 38
39 d Commercial liability (5 .2) . 3d 1234567890 1234567890 1234567890 35% 123456789039
40 40
41 Premiums for Fire State Aid 4 Inland marine (9) . . . . . . . . . . . 4 15% 41
1234567890 1234567890 1234567890 1234567890
42 42
43 5 Earthquake (12) . . . . . . . . . . . . 5 1234567890 1234567890 1234567890 15% 123456789043
44 44
45 6 Aircraft physical damage (22) . 6 1234567890 1234567890 1234567890 10% 123456789045
46 46
47 7 Other fire, lightning, sprinkler 47
48 leakage, extended coverage . . 7 1234567890 1234567890 1234567890 % 123456789048
49 49
50 8 Add lines 1 through 7, 50
51 column E . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8123456789051
52 52
53 No payment For informationaldue. purposes only. 53
54 Attach this report to your Form M11. Keep a copy for your records. 54
55 I declare that this return is correct and complete to the best of my knowledge and belief. 55
56 56
57 Authorized Signature Title Date Daytime Phone 57
X I authorize the Minnesota
58 Department of Revenue to 58
59 SignatureNAMEPreparerof HEREXXXXXXXXXXNAMEPrint Name Preparerof HERE 12051966Date Daytime6126781234Phone discuss this tax return with 59
the preparer .
Sign Here
60 NAME HEREXXXXXXXXXX NAME HERE 12051966 6126781234 60
61 Mail to: Minnesota Department of Revenue, Mail Station 1780, 600 N. Robert St., St. Paul, MN 55146-1780. 61
62 Do not send to the Minnesota Department of Commerce . 62
63 63
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54 56 58 60 62 64 66 68 70 72 74 76 78 80 82 84 86
65 65