Enlarge image
Tab to navigate within form. Use mouse to check Save Print Clear
applicable boxes, press spacebar or press Enter.
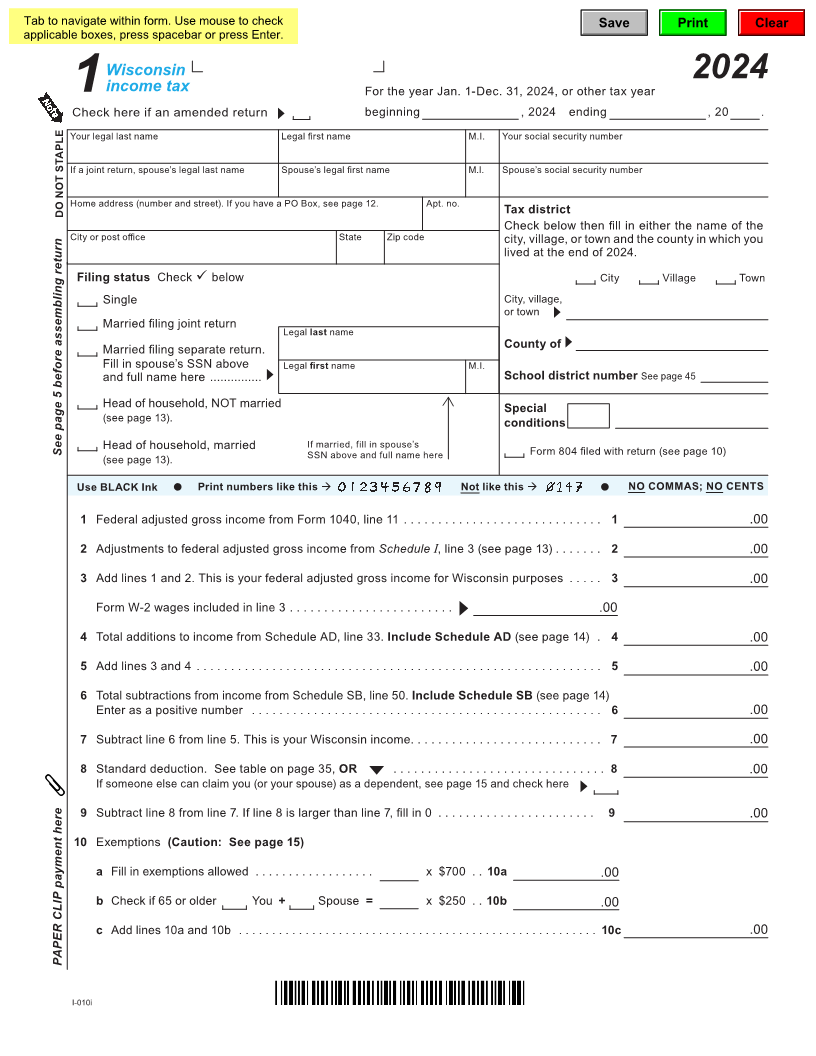
Wisconsin
income tax 2024
For the year Jan. 1-Dec. 31, 2024, or other tax year
1
Check here if an amended return beginning , 2024 ending , 20 .
Your legal last name Legal first name M.I. Your social security number
If a joint return, spouse’s legal last name Spouse’s legal first name M.I. Spouse’s social security number
Home address (number and street). If you have a PO Box, see page 12. Apt. no.
DO NOT STAPLE Tax district
Check below then fill in either the name of the
City or post office State Zip code city, village, or town and the county in which you
lived at the end of 2024.
Filing status Check below City Village Town
Single City, village,
or town
Married filing joint return
Legal last name
Married filing separate return. County of
Fill in spouse’s SSN above Legal first name M.I.
and full name here ............... School district number See page 45
Head of household, NOT married Special
(see page 13). conditions
See page 5 before assembling return Head of household, married If married, fill in spouse’s Form 804 filed with return (see page 10)
(see page 13). SSN above and full name here
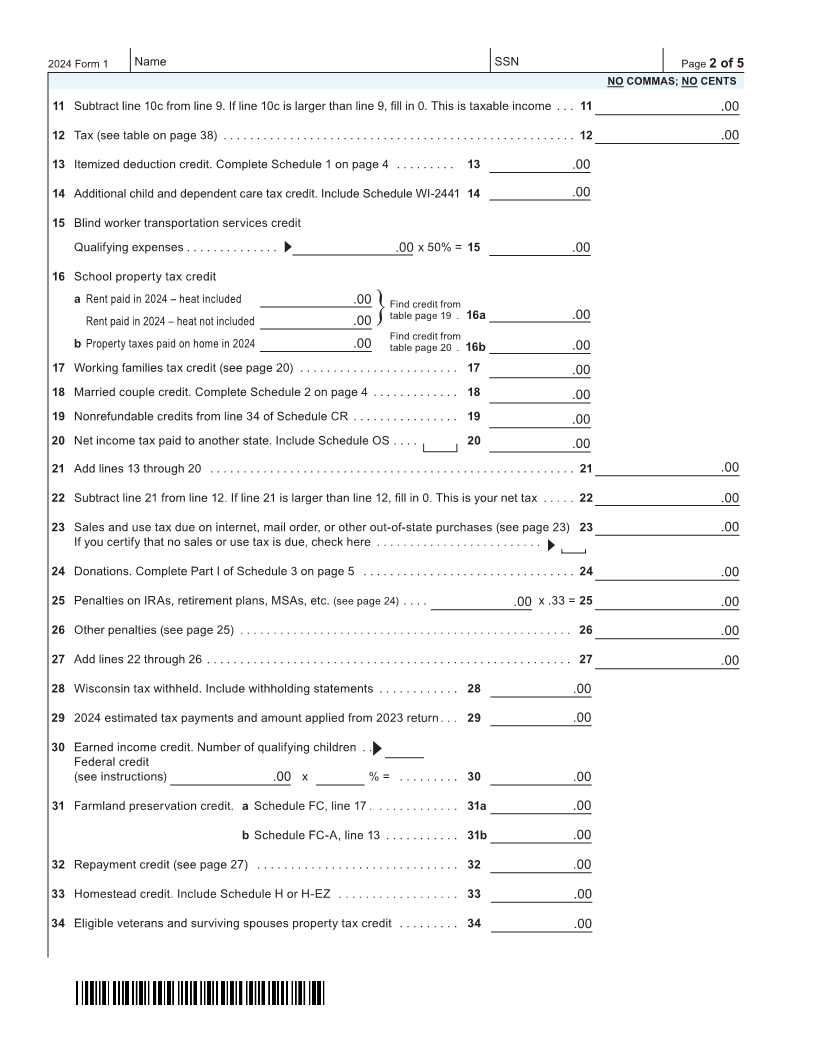
Use BLACK Ink Print numbers like this Not like this NO COMMAS; NO CENTS
1 Federal adjusted gross income from Form 1040, line 11 ............................. 1 .00
2 Adjustments to federal adjusted gross income from Schedule I, line 3 (see page 13) ....... 2 .00
3 Add lines 1 and 2. This is your federal adjusted gross income for Wisconsin purposes ..... 3 .00
Form W-2 wages included in line 3 ........................ .00
4 Total additions to income from Schedule AD, line 33. Include Schedule AD (see page 14) . 4 .00
5 Add lines 3 and 4 ........................................................... 5 .00
6 Total subtractions from income from Schedule SB, line 50. Include Schedule SB (see page 14)
Enter as a positive number ................................................... 6 .00
7 Subtract line 6 from line 5. This is your Wisconsin income ............................ 7 .00
8 Standard deduction. See table on page 35, OR ............................... 8 .00
If someone else can claim you (or your spouse) as a dependent, see page 15 and check here
9 Subtract line 8 from line 7. If line 8 is larger than line 7, fill in 0 ....................... 9 .00
10 Exemptions (Caution: See page 15)
a Fill in exemptions allowed .................. x $700 . . 10a .00
b Check if 65 or older You + Spouse = x $250 . . 10b .00
c Add lines 10a and 10b ...................................................... 10c .00
PAPER CLIP payment here
I-010i